ECR 2018 / C-1627

Conventional radiology in the study of dysphagia. The role of Barium esophagogram and Videofluoroscopic oropharyngeal swallow study.
Congress:
ECR 2018
Poster Number:
C-1627
Type:
Educational Exhibit
Keywords:
Swallowing disorders, Motility, Contrast agent-oral, Barium meal, Conventional radiography, Gastrointestinal tract
Authors:
F. J. Azpeitia Armán, R. M. Lorente Ramos, C. Oliva Fonte, M. P. Gete García, T. Collazo Lorduy; Madrid/ES
DOI:
10.1594/ecr2018/C-1627

Table 1:
Table of contents

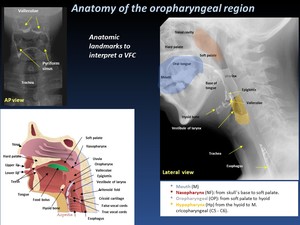
Fig. 1:
Anatomy of the oropharyngeal region

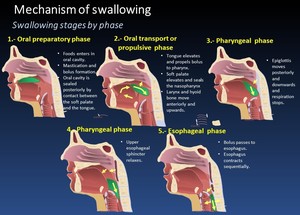
Fig. 2:
Mechanism of swallowing
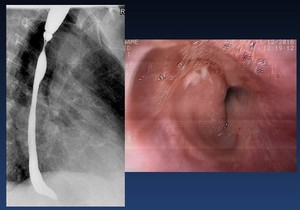
 aortic arch, (LMB) left mainstem bronchus, and (LA) left atrium on the esophagus.")
Fig. 4:
Oblique view of a normal barium swallow shows the normal impressions made by...

Fig. 6:
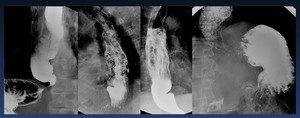
Barium swalow: doublé, contrast, simple contrast and mucosal relief
 view are the
walls of the pharynx laterally, the nasopharynx superiorly, and the cervical esophagus
inferiorly.")
Fig. 8:
The boundaries of the fluoroscopy field in the lateral view are the lips...

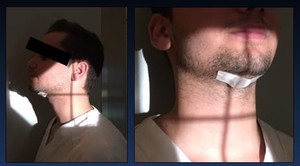
Fig. 7:
Patient preparation prior to study. A radiopaque disk or coin is secured to...

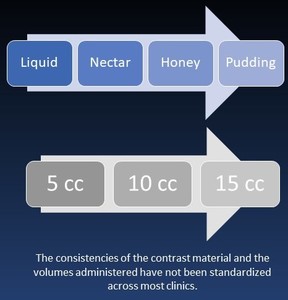
Fig. 9:
The consistencies of the contrast material and the volumes administered have...

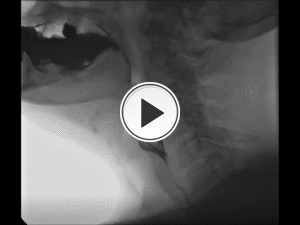
Fig. 10:
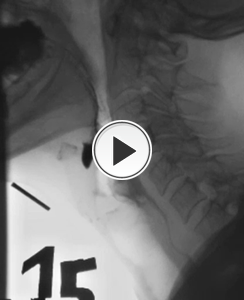
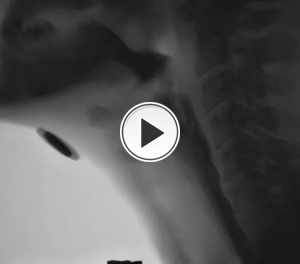
Video capture of a lateral view VFSS. Weakness of the lip seal results in...

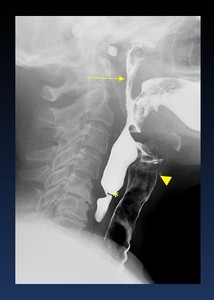
Fig. 12:
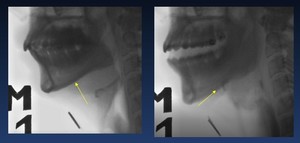
Videocapture VFSS.- Premature spillage of liquid during the oral phase (arrows
 of liquid bolus into nasopharynx caused by impaired velopharyngeal closure.
Aspiration of barium entering the trachea (arrowheads).
Stricture at Killian mouth (*)")
Fig. 13:
Nasal regurgitation (arrow) of liquid bolus into nasopharynx caused by impaired...

Fig. 15:
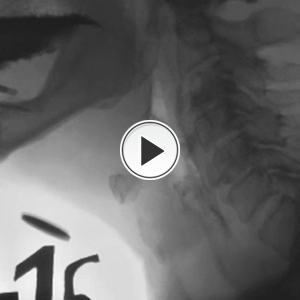
VFS Honey 15 cc.- Normal Hyoid movement

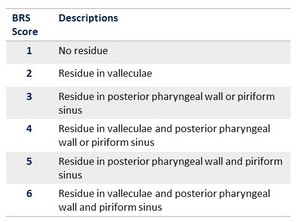
Table 2:
Residuo score
 without aspiration, the contrast remains above the true vocal folds
b.- Gross aspiration of barium entering the trachea")
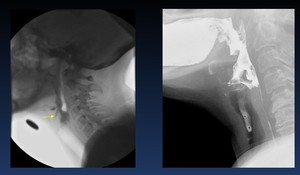
Fig. 18:
A.- Video capture of a lateral view of a laryngeal penetration (arrow) without...

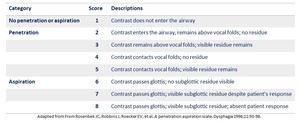
Table 3:
A penetration aspiration scale

Fig. 19:
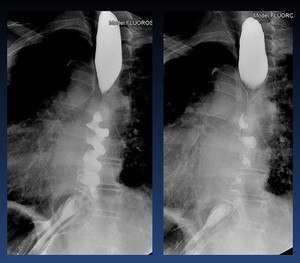
Tertiary contractions, presbyesophagus

Fig. 20:
Diffuse esophageal spasm

Fig. 21:
Achalasia. Dilation with absent peristalsis and Smooth tapering at esophageal...
 arrows without aspiration")
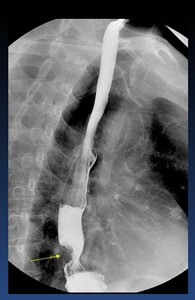
Fig. 22:
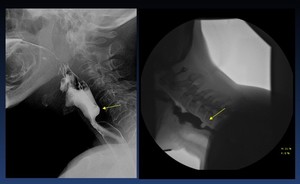
Lateral view and Video capture of a lateral view of a cricopharyngeal bar...
")
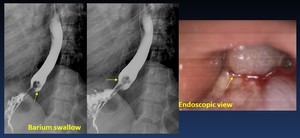
Fig. 23:
Cervical esophageal web (arrow)
")
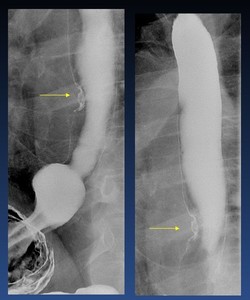
Fig. 24:
Zencker´s diverticulum (arrows)
")
Fig. 25:
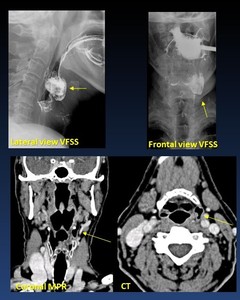
Pharyngocele/ Pharyngeal Diverticula. 67 yo woman with dysphagia. Left...

Fig. 26:
Esophageal Leiomyoma

Fig. 27:
Esophageal Hyperplastic Polyp

Fig. 28:
early esophageal carcinoma

Fig. 29:
Distal esophagus Carcinoma

Fig. 30:
Squamous cell carcinoma
 with esophagitis and Barret,s esophagus")
Fig. 31:
Gastroesophageal reflux disease (GERD) with esophagitis and Barret,s esophagus

Fig. 32:
Peptic esophageal stenosis. Foloww up
")
Fig. 33:
Benign caustic stenosis (arrow)
 following caustic ingestion and esophagitis")
Fig. 34:
Upper stricture (arrow) following caustic ingestion and esophagitis

Fig. 35:
Eosinophilic esophagitis. Stricture

Fig. 36:
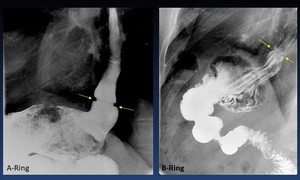
Lower esophageal rings

Fig. 37:
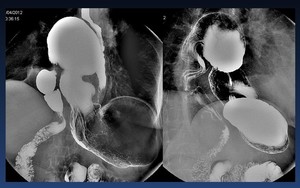
Sliding hernia

Fig. 38:
Paraesophageal hernia

Fig. 39:
Giant esophageal diverticulum

Fig. 40:
Esophageal diverticula

Fig. 41:
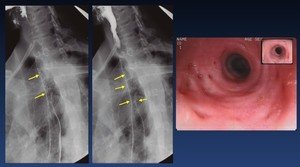
Esophageal intramural pseudodiverticulosis

VFS.- Frontal view showing anterior osteophytes in the region of C 3, C 5 causing narrowing of the hypopharynx and retention in left pyriform sinus.")
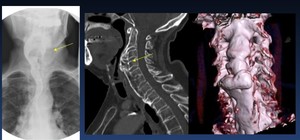
Fig. 42:
Cervical osteophyte C3-C4 narrowing the esophageal lumen (arrow)
VFS.- Frontal...

Fig. 43:
intrathoracic goiter

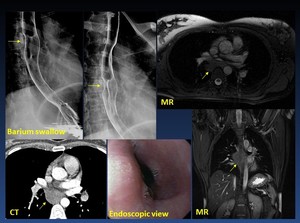
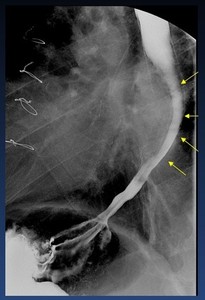
A 84-year-old female patient with left atrial dilatation, presenting with dysphagia and weight loss")
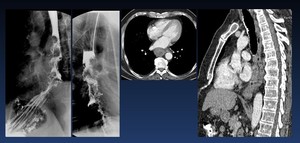
Fig. 44:
Dysphagia secondary to left atrial dilatation (arrows)
A 84-year-old female...

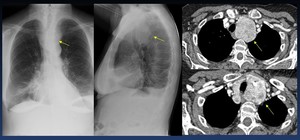
Fig. 45:
Compression and esophageal ulceration caused by lung cancer
 with clinical dysphagia.")
Fig. 46:
67-yo man total laryngectomy with implantation of a phonatory prosthesis (*)...
. Difficulty in esophageal emptying and dysphagia. Note the esophageal dilation.")
Fig. 47:
Laparoscopic nissen Fundoplication (arrows). Difficulty in esophageal emptying...

Fig. 48:
2016.- Gastric band too tight with secondary dilatation of esophagus and slow...