We will be discussing the myriad manifestations of tuberculosis on computed tomography according to the systems involved such as the peritoneum,
lymphatic,
gastrointestinal,
visceral and genitourinary systems.
[3,5,6,7]
Peritoneum
Involvement of the peritoneum which includes the peritoneal cavity,
mesentery and the omentum,
is the most common presentation of abdominal tuberculosis.[2,7] It results from hematogeneous spread of the disease or can be secondary to rupture of mesenteric lymph nodes,
gastrointestinal dissemination or tubercular salpingitis.[7] Tubercular peritonitis is categorized into three types - dry,
wet and fibrinous.[5,7].
1) Wet peritonitis: Most common type,
seen in about 90% of the cases.
It is characterized by free or loculated fluid collections.[5,7]
The ascitic fluid is of high density (20-45 HU) due to the proteinaceous content of the inflammatory exudates which is characteristic of tuberculosis.[5]
It may or may not be associated with smooth and regular peritoneal thickening,[7] however associated peritoneal enhancement is usually present.[5]Fig. 1

Fig. 1: Wet peritonitis: Moderate amount of free fluid with mild smooth thickening and enhancement of the peritoneum is seen.
2) Dry / plastic peritonitis: It is characterized by fibrinous peritoneal and mesenteric thickening,
dense adhesions,
caseous nodules and mesenteric lymphadenopathy.[5,7] Fig. 2

Fig. 2: Dry Peritonitis: Diffuse smooth thickening of the peritoneum and linear striations involving mesentery with necrotic lymphadenopathy is seen.
Mesenteric and omental involvement may range from mild linear striations,
vascular engorgement,
star-shaped appearance,
fat densification to more extensive involvement showing diffuse infiltration of the mesenteric leaves with micro (<5mm) or macro( >5mm) nodules.[7] Fig. 3 Fig. 4
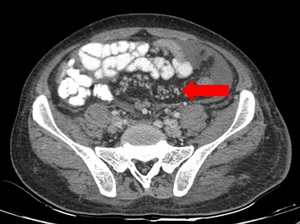
Fig. 3: Mesenteric involvement: Multiple small nodules are noted infiltration the mesentery as shown by arrow.
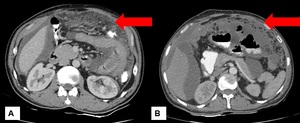
Fig. 4: Omental changes : Diffuse thickening and densification of the omentum is noted in both the images(arrows).
Peritoneal thickening in tubercular peritonitis should be differentiated from peritoneal thickening occuring in peritoneal carcinomatosis which is irregular and nodular as compared to smooth and regular seen in tuberculosis.[7] Fig. 5
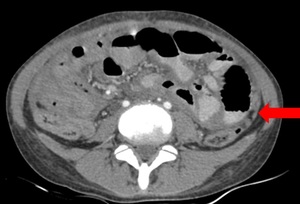
Fig. 5: Pertioneal thickening: Mild irregular and nodular peritoneal thickening (arrow) with moderate ascites seen in a case of peritoneal carcinomatosis.
3) Fixed/ fibrotic peritonitis: This is the rare type of peritonitis which is characterized by omental thickening,
matting of the bowel loops and loculated ascites.[5,7]
Sclerosing encapsulating peritonitis or abdominal cocoon is a type of fibrinous peritonitis which may invariably present as acute or subacute intestinal obstruction with or without an abdominal mass .
It is usually diagnosed incidentally at laparotomy.[10]
Computed tomography demonstrates fixed,
adherent and centrally displaced bowel loops encased by a thick enhancing fibrocollagenous sac with ascites.[10] Fig. 6
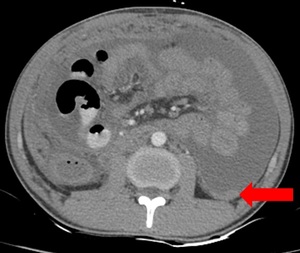
Fig. 6: Abdominal cocoon: Multiple small bowel loops are seen clustered in the center of the abdomen encased by a thick sac(arrow).
Combination of features from any of the types of peritonitis discussed above can be found.
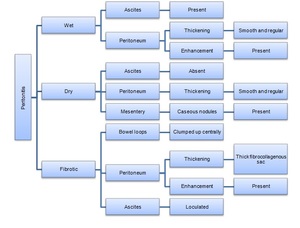
Fig. 7: Summary of the peritoneal involvement of tuberculosis.
Lymphatic tuberculosis
Lymph node involvement is another common manifestation of abdominal tuberculosis.[5] It is mostly associated with gastrointestinal tuberculosis though it may be the only sign of disease such as in the periportal region.[7]
Pattern of involvement usually follows the drainage of the affected organs after ingestion of the infected material.[5,7] Thus lymphadenopathy involving the mesenteric,
celiac,
porta hepatis peripancreatic and paraaortic lymph nodal chain may be seen when the ileocecal,
jejunal,
ileal and right colonic regions are involved.[7]
Other less common modes of transmission are haematogenous spread and contiguous spread from adjacent affected organs.[5]
On computed tomography,
tubercular lymphadenopathy typically manifest as multiple conglomerate of enlarged nodes with hypoattenuation in the center and hyperattenuation in the periphery after intravenous contrast injection which suggests presence of intranodal necrosis.[2,5,7]
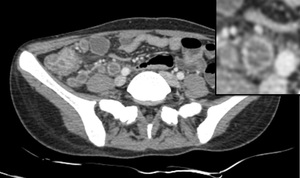
Fig. 8: Necrotic lymphadenopathy: Multiple enlarged hypodense lymph nodes with peripheral enhancement (Zoomed image) are noted in the right iliac fossa. Also noted is thickening of the adjacent bowel loops.
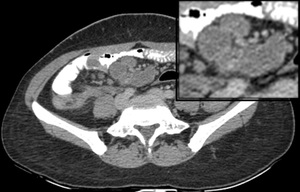
Fig. 9: Conglomerate necrotic lymphadenopathy: Multiple enlarged conglomerate (zoomed image) of hypodense lymph nodes with peripheral enhancement are noted in the mesentery.
Other patterns such as increase in number of normal sized nodes or large localized nodes in clusters or conglomerates Fig. 9 and inhomogeneous enhancement can also be found.[5,7]
Calcification within the nodes can be occasionally seen,
which is considered as an indicator of adequate response to the treatment.
Fig. 10

Fig. 10: Calcified abdominal lymph nodes: Multiple calcified mesenteric pre aortic, para aortic and celiac group of lymph nodes are noted in a follow up case of tubercular lymphadenopathy.
Common differentials of tubercular lymphadenopathy are lymphoma,
metastasis,
pyogenic infection and Whipple's disease.[7]
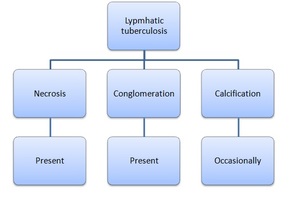
Fig. 11: Summary of the lymphatic involvement of tuberculosis.
Gastrointestinal tuberculosis
Tuberculosis can involve any part of gastrointestinal tract,
but ileocecal region is most commonly involved,
followed by terminal ileum and cecum,
ascending colon jejunum,
descending colon and rectum.
[2,3,5,6,7] The esophagus,
stomach and duodenum are rarely involved.[5]
Ileo-cecal tuberculosis
Ileocecal region along with the terminal ileum and the caecum accounts for about 90% of the cases of intestinal tuberculosis.[2,7] This region is commonly affected due to physiological stasis,
abundance of lymphoid tissue,
increased rate of absorption and closer contact of the bacteria with the mucosa of this region.[5]
It occurs in three forms,
namely,
ulcerative,
hypertrophic,
and ulcerohypertrophic,
with the ulcerative type being the most common.[3] Ulcerative disease usually shows transverse ulcers,
which are often superficial and heal by fibrosis.[3] Hypertrophic form shows thickening and mass-like appearance of bowel associated with scarring and fibrosis.[3]
Clinically patient presents with colicky abdominal pain,
weight loss,
loss of fever and vomiting.[2,5]
Computed tomography shows circumferential wall thickening of the terminal ileum,
ileocecal junction and cecum with narrowing of the lumen,
dilatation of the proximal bowel segment and associated mesenteric lymphadenopathy.[3,5,7] Fig. 12
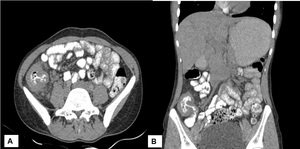
Fig. 12: Ileocecal tuberculosis: (A) Axial post contrast image shows thickening of the ilieocecal junction and cecum. (B) Coronal reformatted images shows abnormal thickening of the ileocecal junction and cecum.
It can also show a heterogeneous mass consisting of thickened ilieocaecal valve,
lymph nodes and adherent or matted bowel loops and mesentery.[7]
The intestinal wall thickening found in tuberculosis is usually homogeneous without stratification and shows enhancement on post contrast study in acute stage.[3] Fig. 13 Chronic disease may present as strictures which are short segments of wall thickening without wall enhancement or stratification and with proximal bowel dilatation.[3,5]
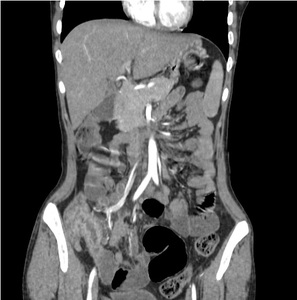
Fig. 13: Ileocecal junction: Abnormal enhancement of the thickened ileocecal junction is noted.
Acute to subacute obstruction is the commonest complication of ileo-cecal tuberculosis which occurs secondary to stricturous narrowing and adhesions of the bowel loops.(Discussed in next section)
Typically,
the site of involvement in tuberculosis is single.
When multiple sites of involvement are seen differentiation from Crohn's disease becomes difficult.[3,5]
Computed tomography nicely depicts the bowel wall and extra intestinal changes however mucosal changes are better appreciated on barium studies or CT enteroclysis.[3,5]
Colo-rectal tuberculosis
Isolated involvement of colon is seen in only 10.8%.[5] Caecum is most commonly involved.
Apart from caecum other sites of colonic involvement are ascending colon followed by transverse colon,
rectum and descending colon.[11] Multifocal involvement is seen in 28%-44% of cases with colorectal TB.[5]
Clinically patient may present with abdominal pain followed by constipation,
loss of weight and appetite and altered bowel habits.
Haematochezia is seen in rectal tuberculosis.[5,7]
Radiological features are presence of strictures followed by features of colitis (thickened and hypervascular bowel wall) and polypoidal lesions.[5]

Fig. 14: Ascending colon and caecal tuberculosis: Abnormal enhancing wall thickening is noted involving the ascending colon and caecum.
Anal tuberculosis may manifest as ulcerative proctitis,
ischiorectal abscess(Fig. 15),anal fissure or stricture.[12]
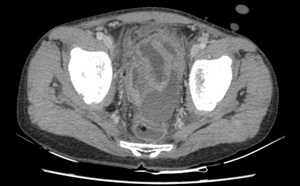
Fig. 15: Rectal collection : Well defined loculated fluid collection in the recto-vesicle pouch and along the wall of the rectum.
Complications in the form of perforations and fistulae can be seen in upto 18.9% of cases.[5]
Various conditions like Crohn’s disease,
amebic colitis,
pseudomembranous and ischemic colitis,
and malignancy form the differential diagnosis of tubercular colitis.[3,5]
Hence the diagnosis of colorectal TB should be based on high index of suspicion and should be proven by colonoscopy guided biopsy and demonstration of caseating granulomas in the tissue.
Jejunal and ileal tuberculosis
Isolated jejunal involvement is rare and is seen in concomitance with ileal involvement in the form of single or multiple short or long segment strictures.[3,5,7]
Ulcerative form is more common than hypertrophic form,
with stellate or linear ulcer extending perpendicular to the long axis of the bowel.[2,5,7]
The clinical features of small intestinal TB are non specific,
and the patients usually present with colicky abdominal pain and vomiting.[5]
Radiologically,
jejunal involvement may manifest as abnormal wall thickening(Fig. 16) and multiple small segment narrowing/strictures(Fig. 17),
which may lead to small bowel obstruction.

Fig. 16: Jejunal tuberculosis: Long segment wall thickening is noted involving the jejunal loops causing mild luminal narrowing with adjacent necrotic lymph nodes.
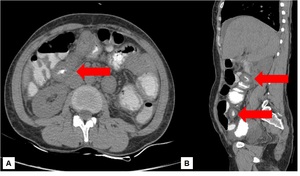
Fig. 17: Multiple strictures: Short segment small bowel wall thickenings are noted involving multiple loops (arrows). Though no air fluid levels are noted.
In areas of high prevalence such as India,
tubercular enteritis is the most common cause of small bowel obstruction and the second commonest cause of perforation after typhoid fever.[5,13]
Gastro-duodenal tuberculosis
Gastric involvement is very rare (0.4%-2%) because of the bactericidal property of the gastric acid,
scarcity of lymphoid tissue in gastric wall and thick intact gastric mucosa.[5]
Usually occurs secondary to spread from adjacent lymph nodes or hematogeneous spread.[5]
Commonly seen along the lesser curvature and pylorus.[5]
Radiological features are non specific and mimic benign ulcer in ulcerative form,
though outlet obstruction may be seen due to the inflammatory changes,
fibrosis or enlarged lymph nodes.[5] Diagnosis is usually by upper endoscopy.
Duodenal involvement is also rare accounting for 2% of the cases.[5]
It can be of extrinsic or intrinsic type.
Extrinsic form is more common and is usually seen secondary to the lymphadenopathy in the C-loop of the duodenum.
The intrinsic form can be ulcerative,
hypertrophic or ulcero-hypertrophic and is complicated by formation of strictures or fistulas.[5]
3rd part of duodenum is commonly involved.
Computed tomography demonstrates luminal narrowing,
mural thickening of duodenum and also adjacent lymph nodal masses causing compression.[5]
Visceral tuberculosis
Liver
Isolated liver involvement is uncommon and it is usually associated with infection of the other organs such as spleen.[7,14]
Two forms of hepatic tuberculosis are seen- miliary and macronodular.[7,14]
Miliary /micronodular form:
It is seen when there is hematogenous dissemination of infection leading to diffuse involvement of the liver.[7]
It is commonly observed with miliary form of pulmonary tuberculosis.[7,14]
On computed tomography,
one may or may not appreciate the small miliary nodules measuring 0.4-2mm in diameter but the liver may be enlarged in size showing homogeneous or heterogenous appearance.[7,14] Fig. 19
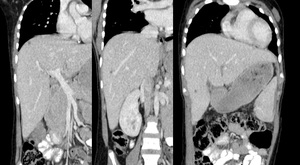
Fig. 19: Micronodular abscess liver: Multiple small non enhancing lesions are seen scattered throughout the hepatic parenchyma in a known case of miliary tuberculosis.
Macronodular form:
The macronodular presentation is a rare manifestation.
It is related to dissemination through the portal vein or hepatic artery from the infected para aortic or the portal nodes.[7,14]
On computed tomography,
hypodense lesions measuring between 1 and 3 cm in diameter or single lesion may be seen in an enlarged liver.
In acute stages it mimics abscess,
however calcifications may arise in the chronic phase of the disease.[7,14]
Common differentials include: Pyogenic or amoebic liver abscess,
Hodgkins disease or metastasis.
Gall bladder and biliary tree is rarely involved and the diagnosis is usually done postoperatively by histopathology.
Spleen
Generally seen in patients with severe,
disseminated tuberculosis such as immunocompromised and HIV positive patients.[7]
As for hepatic lesions,
splenic lesions are also of two types miliary and macronodular.[7]
Miliary type - Usually manifests as moderate splenomegaly,
with minute hypodense lesions seen on/at computed tomography.[7] Fig. 20

Fig. 20: Micronodular abscess spleen: Multiple small non enhancing lesions are seen scattered throughout the splenic parenchyma in a known case of miliary tuberculosis.
Macronodular type - Seen either as multiple or solitary,
rounded or ovoid hypodense nodules/collections. Fig. 21 This form is seen in 15% of HIV positive patients with tuberculosis.
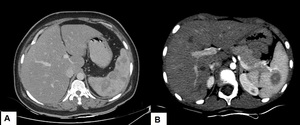
Fig. 21: Splenic macronodular abscess: (A) Multiple hypodense non enhancing abscesses are noted in the splenic parenchyma. (B) Thick walled peripherally enhancing abscess seen in a proven case of tuberculosis.
Calcifications may be seen in chronic or treated cases.
Fig. 22
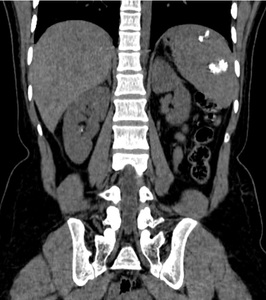
Fig. 22: Splenic calcified granulomas: Multiple variable sized intraparenchymal calcified lesions are seen scattered in the spleen in a treated case of tuberculosis.
Differential diagnosis include: Lymphoma,
Kaposi's sarcoma,
metastasis,
sarcoidosis,
bacillary angiomatosis,
pyogenic/fungal abscesses,
histoplasmosis and Pneumocystis carini infection.[7]
Pancreas
Tubercular involvement of pancreas is extremely rare,
though can be involved in miliary stage of the disease.[7]
Lesions located commonly in the head of pancreas and less common in body or tail.
On imaging,
they appear as hypodense intrapancreatic collection/ complex mass with associated peri-pancreatic lymphadenopathy.
Fig. 23 [7]
Differentials include: Pancreatic mucinous cytstic neoplasm,
pancreatitis or abscess.[7]
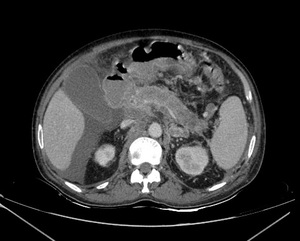
Fig. 23: Pancreatic tuberculosis : Abnormal hypodense non enhancing areas are noted in the head and body of pancreas with mild fat stranding,necrotic peripancreatic lymphadenopathy and ascites. Patient had pulmonary tuberculosis with miliary spread of the disease.
Adrenal glands
Adrenal tuberculosis is the most important cause of adrenal insufficiency,
especially in the developing world.
In developed world,
it contributes 10% of the cases of addisons disease.[7,15]
Clinically patient presents with a generalized weakness and debility,
remarkable feebleness of the heart’s action,
irritability of the stomach and a peculiar change of the color in the skin.[15]
Radiologically,
patient presents with increase in the size of the glands,
central hypodensity Fig. 24 and either unilateral or bilateral calcifications.
Atrophy and calcifications may be seen in previously treated patients.[7,15]
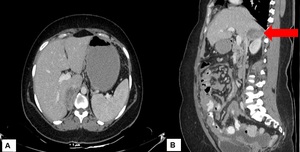
Fig. 24: Adrenal tuberculosis: (A) Well defined peripherally enhancing multiseptate collection in the right suprarenal region seen arising from the right adrenal gland (B) Coronal reformatted image.
Differentials include metastasis,
primary neoplasm,
hemorrhage and lymphoma.[7]
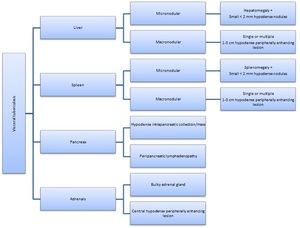
Fig. 25: Summary of visceral tuberculosis.
Genitourinary tuberculosis
Kidneys
Renal tuberculosis is not uncommon and occurs secondary due to hematogeneous spread of the infection from the lungs.[7] Mycobacterium lodges at the corticomedullary junction and forms inactive granulomas in the papilla which remain latent for years.
Reactivation occurs when host immunity is compromised causing papillitis.[7]
Computed tomography shows spectrum of findings including multiple small poorly enhancing nodules,uneven caliectasis and calcification.[16]
In the early stages,
papillary necrosis occurs (single or multiple) resulting in uneven caliectasis. [16]
With disease progression, generalised or focal hydronephrosis with wall thickening and enhancement and poor enhancement of the renal parenchyma occurs.[16] Fig. 26
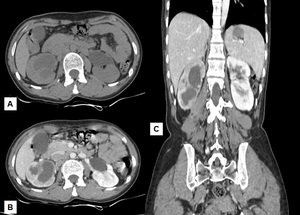
Fig. 26: Renal Tuberculosis: (A) Hypodense area is noted involving the posterior cortex of the lower pole and anterior cortex of the mid pole of right kidney with mild hydronephrosis. (B) Poor enhancement of the right kidney with peripherally enhancement of the cystic areas. (C) Coronal reformated images also shows right psoas abscess and hypodense lesion in the spleen.
In the end-stage disease, there is thinning of the renal parenchyma,
mimicking multiple thin walled cysts,
later amorphous dystrophic calcification involving the entire kidney (known as putty kidney) can be seen.
[16]
Ureters and bladder
Ureters are involved by contiguous spread of infection from the bladder or the kidneys.
In early stages,
computed tomography shows dilatation,
irregular thickening and enhancement of the urothelium.[7,16] Fig. 27 In later stages,
ureteral stenosis,
shortening,
and ureteral calcifications may be seen.[7]

Fig. 27: Ureteric tuberculosis: Mild abnormal nodular thickening is noted involving the right ureter.
Bladder involvement is result of downward spread of disease along the urinary tract causing mucosal ulceration and edema leading to fibrosis of the muscular layer and mural thickening and subsequent decrease in contractility.[7,16]
On imaging,
the main sign of tuberculous cystitis is a thickened bladder and reduced bladder capacity.[7,16] Fig. 28

Fig. 28: Urinary bladder tuberculosis: Evidence of thickening of the bladder wall with reduced capacity is seen in a known case of renal tuberculosis.
Male genital system
The epididymis,
seminal vesicles and prostate are commonly involved followed by vas deferens,
penis and testes.[7,16]
Routes of spread is hematogenous or direct extension from urinary system.[16]
Epididymitis usually starts at the tail of the epididymis and propagates to involve the entire duct.
Ultrasonography and MRI are helpful to diagnose this condition.[7,16]
Prostatic involvement can be in the form of prostatis or abscess.
Computed tomography may show hypodense lesion with peripheral enhancement.
Few calcific foci can be seen in chronic cases.[7]
Female genital system
Most women with genital tuberculosis present with infertility because fallopian tubes are involved in about 95% of cases.[16]
Tubercular salpingitis typically results in bilateral tubal block with multifocal stricture and calcifications.[7]
Tubo-ovarian abscess can also be found.[7,16]
Endometrial involvement occurs following tubal involvement in 50% of cases and can cause adhesion formation.[16]
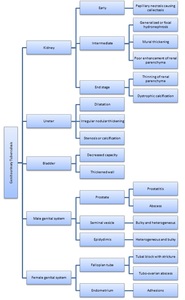
Fig. 29: Summary of genitourinary involvement of tuberculosis.
Others
Iliopsoas muscle involvement can occur as a complication of Potts spine resulting in abscess formation Fig. 30 which may show calcification.[7]
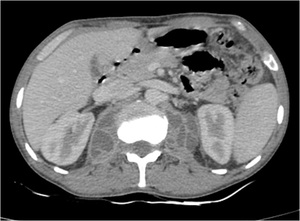
Fig. 30: Bilateral psoas abscess: Ill defined multiloculated collection is seen in bilateral psoas muscles in a case of Potts spine.
Complications can be formation of sinus tract from the collection to the skin surface. Fig. 31

Fig. 31: Sinus tract: An ill defined collection is seen in the right psoas muscle which is piercing the posterior abdominal wall muscles and reaching upto the skin surface.
Abdominal tuberculosis with an acute abdomen
Abdominal tuberculosis presenting as acute abdomen poses an enormous challenge for us,
as our role is not only limited in providing the cause of acute presentation but also aid the surgeon in proper surgical planning by delineating the exact site and extent of involvement.[8]
Various complications which present acute abdomen are small bowel obstruction(47.1%),
perforative peritonitis(31.4%),
acute appendicitis(10%),
abdominal cocoon(4.3%) and others(7.2%).
Small bowel obstruction: Usually seen as a result of single or multiple strictures / adhesions involving the ileum and the ileocecal junction followed by jejunum.
Computed tomography shows multiple air fluid levels with stricture and proximal dilatation of the bowel loop.[3,5,8] Fig. 32 Abnormal enhancement of the bowel wall is also noted.

Fig. 32: Small bowel obstruction – (A) Coronal reformatted image shows circumferential thickening of the bowel loops in the left para aortic region and anterior renal region.(arrow) (B) Sagittal reformated image shows multiple dilated small bowel loops with few air fluid levels within and the thickening of the bowel loop as seen on coronal images.
Perforation: It is the second most common complication,
seen secondary to the ulceration of the bowel wall.
Terminal ileum is the most common site.[17] Usually it is single however multiple perforations may be found.[17]
On computed tomography,
we can see presence of free air in the peritoneum and other features of tuberculosis.
Fig. 33

Fig. 33: Perforation: Extraluminal air in the fluid in the infraumbilical region with omental thickening suggestive of perforation. Patient also had abnormal thickening of the ileal loops just inferior to the air foci.
Acute appendicitis: Result of direct spread of infection from ileocecal junction.
Associated features of tuberculosis such as bowel wall thickening and necrotic lymphadenopathy may be seen.
Abdominal cocoon- Patient presents with a lump in the abdomen due to the matted bowel loops.
(Discussed above) Fig. 6
Prompt diagnosis and management of these acute conditions and their underlying cause is necessary to reduce morbidity and mortality.



 with moderate ascites seen in a case of peritoneal carcinomatosis.")

.")
.")

 are noted in the right iliac fossa. Also noted is thickening of the adjacent bowel loops.")
 of hypodense lymph nodes with peripheral enhancement are noted in the mesentery.")


 Axial post contrast image shows thickening of the ilieocecal junction and cecum. (B) Coronal reformatted images shows abnormal thickening of the ileocecal junction and cecum.")




. Though no air fluid levels are noted.")


 Multiple hypodense non enhancing abscesses are noted in the splenic parenchyma. (B) Thick walled peripherally enhancing abscess seen in a proven case of tuberculosis.")


 Well defined peripherally enhancing multiseptate collection in the right suprarenal region seen arising from the right adrenal gland (B) Coronal reformatted image.")
 Hypodense area is noted involving the posterior cortex of the lower pole and anterior cortex of the mid pole of right kidney with mild hydronephrosis. (B) Poor enhancement of the right kidney with peripherally enhancement of the cystic areas. (C) Coronal reformated images also shows right psoas abscess and hypodense lesion in the spleen.")




 Coronal reformatted image shows circumferential thickening of the bowel loops in the left para aortic region and anterior renal region.(arrow) (B) Sagittal reformated image shows multiple dilated small bowel loops with few air fluid levels within and the thickening of the bowel loop as seen on coronal images.")



