There are numerous etiologies of a SRPL that could optimally be categorized as shown in the table below:
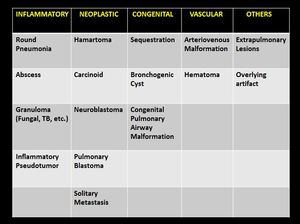
Table 1: Table showcasing the differential diagnosis of a solitary round pulmonary lesion (SRPL) in the pediatric population.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
▪ INFLAMMATORY
▪ Round Pneumonia
The commonest etiology of a SRPL is round pneumonia,
mostly occurring in patients aged <8 years old,
after which age there should be increased suspicion of other underlying causes.
The patient usually presents with cough & fever.
CXR: Soft tissue density solitary lesion,
which doesn’t contain an air-fluid level.
More common posteriorly and in lower lobes.
In this clinical scenario of a child with cough & fever and a round density on CXR CT is not indicated to evaluate for other potential causes.
The patient should be treated with antibiotics and a repeat CXR should be obtained in several weeks.
In 95% of the patients it will resolve on follow-up imaging rather than progressing to lobar pneumonia.

Fig. 1: Round pneumonia. CXR obtained in a 7 year old child presenting with cough and fever shows a solitary round opacification in the upper zone of the right lung. Lab results show elevated white blood cell count and C-reactive protein.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
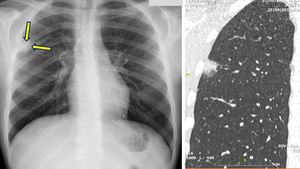
Fig. 2: Eosinophilic pneumonia. CXR showcasing a peripherally located SRPL in the right upper lobe which also demonstrated a halo sign on CT (coronal slice). This proved to be eosinophilic pneumonia.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
▪ Lung Abscess
Uncommon in otherwise healthy children.
They most commonly occur in children with underlying immunodeficiency or complex medical disorders.
Symptoms include fever,
cough and shortness of breath.
CXR: Round cavity with or without an air fluid level,
which appears similar in both frontal and lateral projections.
CT: Perceptible enhancing wall that can be thick and/or irregular.
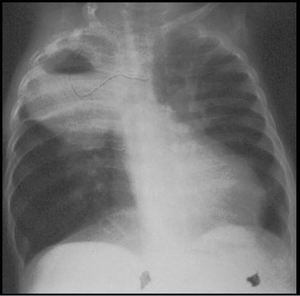
Fig. 3: Lung Abscess. CXR of an immunocompromised patient demonstrates a soft tissue density lesion, with an air-fluid level, in the right upper lobe which was due to a pseudomonas aeruginosa infection.
References: Courtesy of Dr. H. Carty, Alder Hey Children's Hospital, Liverpool, UK
▪ Granuloma - Fungal
Aspergillosis is uncommon in otherwise healthy children and most commonly occurs in immunocompromised children or children with underlying conditions (asthma,
cystic fibrosis or chronic granulomatous disease of childhood).
CXR/CT: Consolidation,
usually with a “halo” sign.
Although rare,
a mycetoma may subsequently form in a preexisting cavity as a superinfection,
in which case an “air crescent” sign can be seen (crescent-shaped air collection surrounding a necrotic mass in the area of consolidation).
The necrotic mass may be mobile.
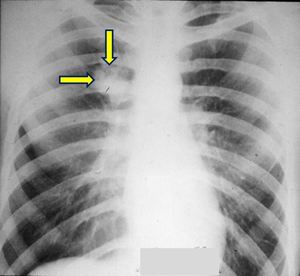
Fig. 4: Fungal Granuloma. Aspergillus infection in an immunocompromised patient appearing as a SRPL in the right upper lobe.
References: Courtesy of Dr. H. Carty, Alder Hey Children's Hospital, Liverpool, UK
▪ Granuloma - Tuberculosis
Most children with tuberculosis have primary disease (clinical infection that follows the first exposure to the organism).
Diagnosis in childhood is difficult to establish clinically due to the lack of physical symptoms. Younger children are more likely to have respiratory symptoms because of the narrower diameter of their airways.
Diagnosis is usually made on the basis of epidemiologic data,
and in the absence of a positive culture,
the strongest evidence is recent exposure to an adult with active disease.
Indirect diagnostic techniques such as the tuberculin skin test and CXR provide supportive information.
The radiologic hallmark of primary tuberculosis in childhood is lymphadenopathy,
typically involving the right hilar and paratracheal nodes and in some patients,
it may be the only intrathoracic finding.
Primary disease presents as an area of consolidation or as a well-defined tuberculoma (SRPL),
accompanied with the previously mentioned lymphadenopathy,
forming the Ranke complex.
Involved lymph nodes commonly show low-attenuation centers,
representing areas of necrosis,
on contrast-enhanced CT.
Calcifications may develop over time at areas of previously formed tuberculomas.
Postprimary TB (mostly occurring in adults) is usually a result of reactivation of latent infection,
with characteristic findings being upper lobe consolidation with cavitation (SRPL),
without adenopathy and effusions.
▪ Pulmonary inflammatory pseudotumors
Inflammatory pseudotumor of the lung,
is a nonneoplastic pulmonary mass lesion of unknown etiology,
which can mimic pulmonary malignancy.
The majority of investigators regard this entity as a variant of an inflammatory repair process that is related with acute & chronic inflammation.
Tends to be clinically silent and detected on routine CXR.
CXR: Usually appears as a solitary,
well-circumscribed round or oval mass.
Calcification and cavitation have been reported.
May involve mediastinum and pleura.
CT: Heterogeneous attenuation with variable patterns of contrast enhancement and calcification.
Atelectasis and pleuritic fluid may be seen unilaterally.

Fig. 5: Inflammatory Pseudotumor (part1). A 12 year old boy was referred to our hospital for further investigation of a lung lesion occurring as an incidental finding. In his recent history a lower respiratory tract infection was mentioned a week prior with fever as much as 40ο C, cough & rhinitis. CXR shows a well demarcated SRPL of heterogeneous density with marked calcifications in the right lower lobe. No previous chest imaging was available. The patient was of normal health status, and his lab results were unremarkable.
References: Courtesy of Dr. G. Passas, General Hospital of Ioannina "G. Hatzikosta"
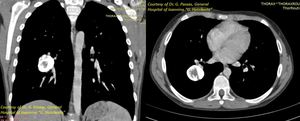
Fig. 6: Inflammatory Pseudotumor (part2). Prior to referral further imaging with CT was performed which showed a well-marginated, round, vividly calcified, 3 cm lesion in the right lower lobe, with no remarkable contrast enhancement.
References: Courtesy of Dr. G. Passas, General Hospital of Ioannina "G. Hatzikosta"
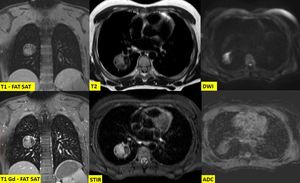
Fig. 7: Inflammatory Pseudotumor (part3). MRI described a cavity with hemorrhagic or protein-rich content, with a calcified capsule and calcified parts mainly at the inner part of the lesion. Absence of fat alienated the possibility of the lesion representing a teratoma or an hamartoma. The most possible diagnosis was that of a chronic inflammation in the setting of a specific infection with the most possible being histoplasmosis and TB. PCR for histoplasma was negative. Ziehl–Neelsen stain for Mycobacterium Tuberculosis was negative. At the 3 month follow up the imaging findings were unchanged. Right lower lobectomy was performed and histopathology made the diagnosis of an inflammatory pseudotumor.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
▪ NEOPLASTIC
▪ BENIGN
▪ Hamartoma
Although rare in children they are the 2nd most frequent benign tumor.
Usually they are clinically silent and the patients are healthy with normal clinical examination & laboratory findings.
As a result detection mostly occurs on routine CXR.
CXR: Sharply demarcated round or lobulated structures usually <3 cm in diameter and peripherally located,
that may increase in size during observation.
CT: Radiological diagnosis is usually based the detection of ‘popcorn-like’ calcifications and/or fat.
MR: Helpful when neither calcification nor fat is demonstrated on CT.
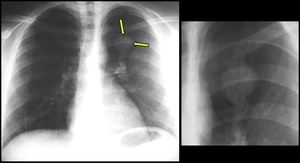
Fig. 8: Pulmonary hamartoma (part1). A 12-year-old boy was referred to our Hospital, when on chest radiography a well-demarcated, lobulated, 3-cm coin shadow was seen in the left upper lobe as an incidental finding.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
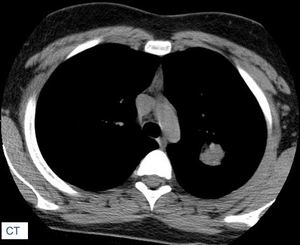
Fig. 9: Pulmonary hamartoma (part2). CT was performed for further evaluation which demonstrated a homogeneous, isoattenuating, lobulated solid mass in the left upper lobe. There was no evidence of fat. Subtle hyperattenuating foci are present peripherally in the lesion, which were suspicious for calcifications.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
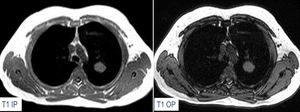
Fig. 10: Pulmonary hamartoma (part3). There is no evidence of fat content on T1-W in-phase and opposed phase sequences (neither on fat-suppressed T1-W), however surgical excision of the lesion revealed a pulmonary hamartoma.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
▪ MALIGNANT
The likelihood of an incidental SRPL in a child representing a primary lung cancer is exceedingly small,
however it should not automatically be assumed as benign.
▪ Carcinoid
The most common primary malignant lung tumors are lesions such as bronchial carcinoids (BCs).
BCs are rare,
well-differentiated malignant neuroendocrine tumours arising from Kulchitsky (neuroendocrine) cell or APUD system cells.
Diagnosis may be delayed due to low clinical suspicion and the varied ways in which BC’s can present.
Symptoms are aspecific,
but their recurrence in a child with obstructive pneumonia localised in the same lobe,
should alert the physician.
CXR/CT: Well-defined ovoid lesions measuring 2- 4 cm,
that often contain calcifications,
are usually located centrally and involve the right middle lobe or lingula.
Atelectasis and mucoid impaction related to endobronchial obstruction can also be seen.
Contrast administration can further assist by detecting enhancement,
mediastinal lymph node involvement and/or metastases.
MRI: Sensitivity not established in the literature.
Useful especially in light of concerns regarding the use of ionizing radiation.
Hyperintense on T2-weighted sequences and on short-inversion- time inversion recovery sequences.
Nuclear medicine: Imaging modalities that target somatostatin receptors directly are often used in combination with anatomic imaging for the assessment of carcinoid and other neuroendocrine tumors.
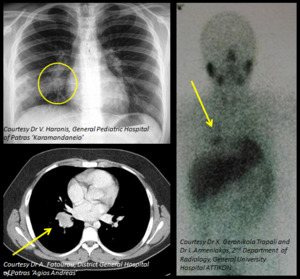
Fig. 11: Carcinoid tumor (part 1). 13 year old boy presenting with recurrent episodes of right lower lobe pneumonia. CXR shows a solitary round pulmonary lesion close to the right hilum with postobstructive pneumonitis. CT shows a homogeneously enhancing lesion of the right lower lobe. Nuclear scan demonstrates a focus of increased uptake of I123 MIBG in the right lower lobe. Uptake of I123 MIBG is seen in tumors originating from neural crest cells (neuroblastoma, neuroganglioma, carcinoid).
References: Dr V. Haronis, General Pediatric Hospital of Patras "Karamandaneio" - Dr A. Fatourou, District General Hospital of Patras "Agios Andreas" - Dr X. Geronikola Trapali and Dr I. Armeniakos, Department of Radiology, University General Hospital of Athens "Attikon"
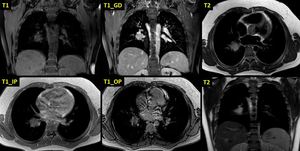
Fig. 12: Carcinoid tumor (part 2). MRI scan in the same patient. The lesion displays low signal in T1 sequences, mild patchy contrast enhancement after intravenous administration of gadolinium and high signal in T2 sequences. There is no decrease in signal intensity in the T1 opposed phase sequences which would document the presence of intracellular fat.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
▪ Neuroblastoma
Tumors of neuroblastic origin arising from the sympathetic nervous system,
typically occurring in infants and very young children.
Intrathoracic disease is less common than intra-abdominal disease.
Presentation can be unusual,
depending on size,
location and mass effect on adjacent structures.
Neurological signs (as a result of infiltration of neural foramina),
as well as atypical respiratory symptoms may be present.
Most commonly will appear as obvious posterior mediastinal mass.
In young children <2 years of age,
a posterior mediastinal mass is neuroblastoma until proven otherwise.
CXR: Round or lobulated lesion.
MRI: Imaging modality of choice (as for all posterior mediastinal lesions).
The classic “dumbbell” appearance (extension of the lesion into the neural foramen) is exquisitely demonstrated on MRI.
CT: Typically heterogeneous with low attenuating areas of necrosis.
Useful for detecting calcifications (80-90% of cases) and bony erosion (rib,
neural foramen).
US: Heterogeneous mass with internal vascularity.
Areas of necrosis appear as regions of low echogenicity.
Calcification may or may not be evident.

Fig. 13: Neuroblastoma. After the detection of this soft tissue density SRPL on a routine CXR, an ultrasound of the chest was performed which described the presence of a paravertebral mass with calcifications which was well demarcated and had a clear transition to the healthy lung parenchyma. There was no coexisting pleural effusion. Further imaging and evaluation proved this to be an intra-thoracic neuroblastoma.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
▪ Pleuropulmonary blastoma
Very rare,
highly aggressive and malignant tumor,
originating from either the lungs or pleura occurring mainly in children <6 years.
Are classified into three groups as:
- cystic (type I),
- mixed (type II),
- solid (type III)
The common presenting symptoms include dry cough,
fever,
dyspnea,
tachypnea,
chest pain,
fatigue,
and respiratory infections that do not resolve with antibiotic therapy.
It is difficult to diagnose preoperatively since the tumor has no characteristic imaging findings and surgical resection is recommended when such malignancy is suspected.
The diagnosis is usually indicated by a CXR which shows a unilateral solid or cystic lesion,
or sometimes a partial or complete opacification of the hemithorax with mediastinal deviation to the contralateral side.
CT & MRI scans reveal extensive involvement of a solid and/or cystic tumor.
▪ Solitary Lung Metastasis
Metastatic disease to the lung is far more common than a primary lung tumor,
with Wilms tumor being the most common primary lesion in infants and children.
Clinical suspicion should be raised in patients with a known primary malignancy.
Atypical imaging features include consolidation,
cavitation,
hemorrhage,
and secondary pneumothorax.
Treated metastases,
osteosarcomas and chondrosarcomas may also contain calcified densities.
▪ CONGENITAL
▪ Bronchopulmonary Sequestration
Rare congenital malformation of the lower respiratory tract consisting of a nonfunctioning lung tissue mass that lacks normal communication with the tracheobronchial tree,
and receives its arterial blood supply from the systemic circulation.
Sequestrations are classified anatomically,
as:
- Intralobar: most common - located within a normal lobe - lacking its own visceral pleura
- Extralobar: located outside the normal lung - has its own visceral pleura.
Clinical presentation depends on type,
size,
and location.
Symptoms vary between respiratory distress,
cyanosis and infection.
US: Most cases are identified on routine prenatal ultrasound examination.
Appears as a well-defined or irregular echogenic homogeneous mass. A pathognomonic feature is a systemic artery from the aorta to the fetal lung lesion detected by color flow Doppler.
CXR: Typically appears as a uniformly dense mass within the thoracic cavity or pulmonary parenchyma. Recurrent infection can lead to the development of cystic areas within the mass.
Air-fluid levels may be seen due to bronchial communication.
CT: Mostly useful for detecting emphysematous changes at the margin of the lesion which are characteristic and may not be visible on CXR.
CTA/MRA: Offers the ability to simultaneously visualize the arterial supply,
venous drainage,
and parenchymal involvement.
The differential diagnosis of BPS includes other cystic lung lesions,
such as Congenital Pulmonary Airway Malformations (CPAM’s) and bronchogenic cysts.
▪ Congenital Pulmonary Airway Malformation (CPAM)
In contrast to BPS,
CPAMs are connected to the tracheobronchial tree,
and are supplied from the pulmonary circulation.
However,
hybrid lesions with histologic characteristics of CPAM and a systemic arterial supply have been reported.
The diagnosis is usually either made on antenatal ultrasound,
or in the neonatal period on the investigation of progressive respiratory distress.
CPAMs can be divided into three types:
- single or multiple air-filled cysts,
often more than 2 cm in size (most common)
- cysts smaller than 2 cm and mixed with solid tissue and
- solitary solid mass (rare)
Radiographic features will vary depending on the type.
CT angiography is able to identify systemic arterial supply if present.
▪ Bronchogenic Cyst
Rare congenital malformations of the bronchial tree that can occur in the mediastinum or be intrapulmonary.
They don’t usually communicate with the bronchial tree,
and are therefore typically not air filled.
Rather,
they contain fluid,
variable amounts of proteinaceous material,
blood products,
and calcium oxalate.
Usually asymptomatic and found incidentally on chest imaging.
CXR: Usually appear as soft-tissue density rounded structures,
sometimes with compression of surrounding structures which could lead to air-trapping and a hyperlucent hemithorax.
CT: Typically appear as well circumscribed spherical or ovoid masses of variable attenuation depending on the amount of internal proteinaceous content.
There is no solid contrast enhancement.
MRI: Mostly homogeneous.
Variable signal intensity depending on protein content.
Fluid-fluid level has also been reported,
attributed to layering of variable fluid content.
▪ VASCULAR
▪ Pulmonary Arteriovenous Malformation (PAVM)
Rare vascular anomalies of the lung,
in which abnormally dilated vessels provide a right-to-left shunt between the pulmonary artery and vein.
Despite most patients being asymptomatic,
affected children may present with cyanosis,
dyspnea,
hemoptysis,
clubbing as well as polycythemia.
A number of modalities are available for the diagnosis of PAVMs,
such as CTA,
MRA and pulmonary angiography all of which will demonstrate enhancement of the feeding artery,
the aneurysmal part and the draining vein.
Pulmonary angiography is the method of choice when percutaneous treatment is also planned.
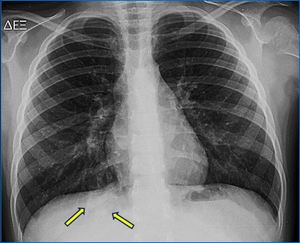
Fig. 14: Pulmonary Arteriovenous Malformation (part1). This patient presented with cyanosis and dyspnea when on chest radiography a soft tissue lesion (SRPL) was detected in the right lower lobe.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
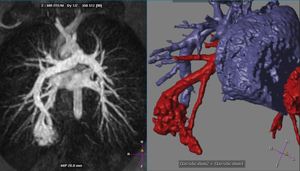
Fig. 15: Pulmonary Arteriovenous Malformation (part2) Further imaging with MR angiography and 3D reconstruction demonstrated a right-to-left shunt between the pulmonary artery and vein (PAVM).
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"
▪ Pulmonary Hematoma
Collections of blood within the alveolar and interstitial space resulting from extensive hemorrhage into a site of parenchymal laceration which are usually round mimicking a SRPL.
Chest trauma is the major cause,
hence history of trauma along with associated injuries (fractures,
pneumothorax etc.) are strong diagnosis indicators.
Follow up will show gradual resolution of the radiologic findings.
▪ OTHERS (Extrapulmonary Lesions)
Extrapulmonary lesions can appear as lung parenchyma lesions on a CXR mimicking SRPL’s.
Such lesions include:
▪ Overlying artifacts
Often they will be very round or other geometric shapes suggesting unnatural cause. Common causes include hair braids,
buttons,
shirt pocket contents,
monitor leads,
and other medical devices.
When in doubt,
removing possible artifact and repeating the CXR,
will help in diagnosis.
▪ Chest Wall Lesion
Rib lesions can appear as round lung lesions on CXR.
Look for rib destruction or erosion to show chest wall origin of lesion.
Clear,
well demarcated boundaries and obtuse angles are also indicative of chest wall origin.
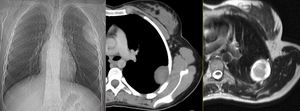
Fig. 16: Extraparenchymal lesion. Chest radiography shows a round/ovoid, soft tissue density in the left hemithorax, which appears to be extraparenchymal and originating from the chest wall due to its clear, well demarcated boundaries and obtuse angles. CT demonstrates a well-defined hypodense solitary round lesion with a broad base to the chest wall. MRI shows surrounding edema and subtle intratumoral cystic necrosis. This lesion proved to be a neurofibroma.
References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"

 in the pediatric population. References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")

. This proved to be eosinophilic pneumonia. References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")


. A 12 year old boy was referred to our hospital for further investigation of a lung lesion occurring as an incidental finding. In his recent history a lower respiratory tract infection was mentioned a week prior with fever as much as 40ο C, cough & rhinitis. CXR shows a well demarcated SRPL of heterogeneous density with marked calcifications in the right lower lobe. No previous chest imaging was available. The patient was of normal health status, and his lab results were unremarkable. References: Courtesy of Dr. G. Passas, General Hospital of Ioannina "G. Hatzikosta"")
. Prior to referral further imaging with CT was performed which showed a well-marginated, round, vividly calcified, 3 cm lesion in the right lower lobe, with no remarkable contrast enhancement. References: Courtesy of Dr. G. Passas, General Hospital of Ioannina "G. Hatzikosta"")
. MRI described a cavity with hemorrhagic or protein-rich content, with a calcified capsule and calcified parts mainly at the inner part of the lesion. Absence of fat alienated the possibility of the lesion representing a teratoma or an hamartoma. The most possible diagnosis was that of a chronic inflammation in the setting of a specific infection with the most possible being histoplasmosis and TB. PCR for histoplasma was negative. Ziehl–Neelsen stain for Mycobacterium Tuberculosis was negative. At the 3 month follow up the imaging findings were unchanged. Right lower lobectomy was performed and histopathology made the diagnosis of an inflammatory pseudotumor. References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")
. A 12-year-old boy was referred to our Hospital, when on chest radiography a well-demarcated, lobulated, 3-cm coin shadow was seen in the left upper lobe as an incidental finding. References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")
. CT was performed for further evaluation which demonstrated a homogeneous, isoattenuating, lobulated solid mass in the left upper lobe. There was no evidence of fat. Subtle hyperattenuating foci are present peripherally in the lesion, which were suspicious for calcifications. References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")
. There is no evidence of fat content on T1-W in-phase and opposed phase sequences (neither on fat-suppressed T1-W), however surgical excision of the lesion revealed a pulmonary hamartoma. References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")
. 13 year old boy presenting with recurrent episodes of right lower lobe pneumonia. CXR shows a solitary round pulmonary lesion close to the right hilum with postobstructive pneumonitis. CT shows a homogeneously enhancing lesion of the right lower lobe. Nuclear scan demonstrates a focus of increased uptake of I123 MIBG in the right lower lobe. Uptake of I123 MIBG is seen in tumors originating from neural crest cells (neuroblastoma, neuroganglioma, carcinoid). References: Dr V. Haronis, General Pediatric Hospital of Patras "Karamandaneio" - Dr A. Fatourou, District General Hospital of Patras "Agios Andreas" - Dr X. Geronikola Trapali and Dr I. Armeniakos, Department of Radiology, University General Hospital of Athens "Attikon"")
. MRI scan in the same patient. The lesion displays low signal in T1 sequences, mild patchy contrast enhancement after intravenous administration of gadolinium and high signal in T2 sequences. There is no decrease in signal intensity in the T1 opposed phase sequences which would document the presence of intracellular fat. References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")

. This patient presented with cyanosis and dyspnea when on chest radiography a soft tissue lesion (SRPL) was detected in the right lower lobe. References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")
 Further imaging with MR angiography and 3D reconstruction demonstrated a right-to-left shunt between the pulmonary artery and vein (PAVM). References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")

 in the pediatric population, as well as helpful clues for diagnosis. References: 2nd Department of Radiology, University General Hospital of Athens "Attikon"")