Indications for Imaging
Both the European Association of Urology [6] and the American Urologic Association [7] have published guidelines outlining the indications for CT in renal trauma.
Both guidelines broadly agree and can be summarised as follows:
1) Haemodynamically unstable patients should be brought directly to
theatre for exploratory laparotomy.
2) Stable patients who have undergone blunt abdominal trauma and either
a. have gross haematuria
OR
b.
have microscopic haematuria AND evidence of shock i.e.
SBP <
90mmHg
should undergo contrast enhanced CT.
3) Stable patients who have undergone blunt abdominal trauma and have
microscopic haematuria only with nothing else to suggest renal injury do
not require imaging.
4) Patients who have undergone trauma where the mechanism of injury
raises a suspicion of renal injury (e.g.
rapid deceleration,
significant blow
to flank,
penetrating trauma,
extensive bruising over flank or rib
fracture) should undergo contrast enhanced CT.
It should be noted that if the mechanism of injury or clinical picture indicates significant injury,
the absence of haematuria should not act as a barrier to imaging as haematuria is only present in a minority of renal trauma and does not correlate with severity of the injury [2].
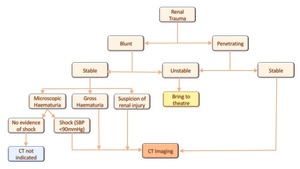
Table 1: Indications for imaging in renal trauma
CT Imaging Protocol
In the setting of renal trauma the imaging protocol used should adequately assess three key components of the kidney: the parenchyma,
vasculature and collecting system.
Imaging usually occurs in the setting of general abdominal trauma for which a trauma protocol is employed to assess for a wide range of injuries.
A trauma protocol for the abdomen involves portal venous phase imaging which corresponds with the corticomedullary phase thus enabling assessment of renal parenchyma.
There is also increasing tendency to include an arterial phase in the trauma protocol to assess for arterial injury [8].
In cases of penetrating trauma preliminary non-contrast images may be of benefit in identifying and distinguishing extravasation from foreign bodies.
If there is suspicion of an injury to the collecting system based on the initial scan,
a delayed or excretory phase should be performed at 10-20 minutes.
Collecting system injury may be indicated on the initial scan by evidence of a laceration which appears to extend to the collecting system or by the presence of perinephric free fluid.
Delayed phase images are also useful in evaluating vascular injuries such as active bleeding and pseudoaneurysm.
Grading System of Renal Injury
The American Association for the Surgery of Trauma (AAST) have developed a scale (Grade I-V) for classifying renal injury in the setting of trauma [9].
This scale is widely used to grade the severity of renal injury and is helpful in planning patient management.
|
Grade of Injury
|
Nature of injury
|
|
I
|
· Contusions
· Subcapsular haematomas
|
|
II
|
· Lacerations <1cm of the renal cortex but not
involving the collecting system
· Perinephric haematomas
|
|
III
|
· Lacerations >1cm of the renal cortex but not
involving the collecting system
|
|
IV
|
· Lacerations extending to involve the cortex,
medulla
and collecting system
· Vascular injuries involving main renal artery/vein
with contained haemorrhage
|
|
V
|
· Vascular injuries involving the main renal artery or
vein with complete devascularisation of the kidney
· Shattered kidney
|
|
*Move up one grade for bilateral injuries grade I-III
|
CT Appearances of Renal Injuries & Management
A. Grade I Injuries
Contusions
|
CT Findings
|
· Poorly defined areas of low attenuation relative to
surrounding parenchyma,
often subtle.
· May have striated appearance due to differential
blood flow through the region and on delayed phase
images may demonstrate a persistent
nephrogram.
· Can be distinguished from segmental infarctions
which are well defined, wedge shaped areas of low
attenuation which do not demonstrate post
contrast enhancement.
|
|
Management
|
· Conservative management.
· No follow up imaging required.
|
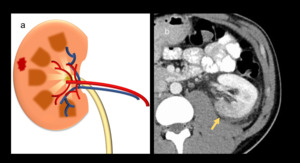
Fig. 2: (a) Illustration of renal contusion. (b) 43 year old male post assault. CT shows an ill-defined area of low attenuation in the left kidney consistent with a renal contusion (Grade I injury).
Subcapsular Haematoma
Subcapsular haematomas are well encapsulated haematomas that develop between the renal parenchyma and the capsule.
|
CT Findings
|
· Typically convex in shape,
appearing as an area of
low attenuation relative to the kidney on
corticomedullary phase imaging.
· As they enlarge they can become biconvex.
· Can cause indentation of the kidney contour.
· On non-contrast studies,
the haematoma appears
hyperattenuating relative to unenhanced renal
parenchyma in the acute phase,
and hypodense
when chronic.
|
|
Management
|
· No intervention required,
they will resolve
spontaneously.
· No follow up imaging required.
· In rare cases the haematoma can enlarge to the
extent that it compresses the underlying kidney and
restricts blood flow.
This in turn activates the RAAS
system with the patient developing secondary
hypertension.
This condition is known as a Page
Kidney.
Initial conservative management is
recommended with surgical intervention being second
line [10].
|
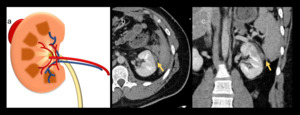
Fig. 3: (a) Illustration of a subcapsular haematoma. (b) & (c) In this 37 year old woman post blunt trauma, a subcapsular haematoma is seen as a well encapsulated area of low attenuation along the lateral border of the left kidney.
A. Grade II/III Injuries
Lacerations (not involving collecting system)
|
CT Findings
|
· Linear or jagged hypodensity extending into
otherwise normal renal parenchyma from the
periphery of the kidney.
· No extension into the collecting system.
· Grade II if < 1cm in length and Grade III if > 1cm.
· Can mimic segmental infarction.
|
|
Management
|
· No intervention required.
· No follow up imaging required.
|
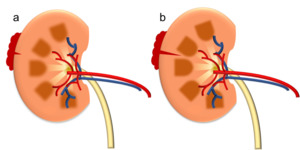
Fig. 4: Illustrations depicting (a) grade II and (b) grade III lacerations.
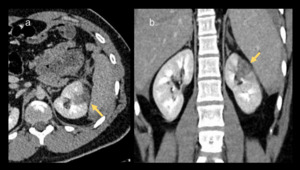
Fig. 5: A 21 year old male post stab wound to the left flank. A grade III laceration to the left kidney is visible as an area of low attenuation extending from the periphery of the kidney (a) & (b).

Fig. 6: 46 year old man post blunt trauma following assault. A linear focus of low attenuation is visible in the lower pole of the left kidney representing a grade III laceration.
Perinephric Haematoma
|
CT Findings
|
· Irregular and poorly defined hyperdense fluid.
· Contained within the retroperitoneum by Gerota’s
fascia
· May extend laterally causing thickening of the lateral
conal fascia
· Unlike subcapsular haematomas,
do not cause
indentation of underlying kidney.
|
|
Management
|
· No intervention required.
· No follow up imaging.
|
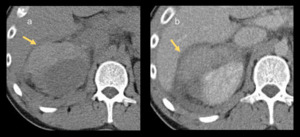
Fig. 7: This 52 year old male involved in an RTA has a right perinephric haematoma. The irregular area of free fluid is hyperattenuating on the non-contrast study (a) indicating it is an acute haematoma.
A. Grade IV Injuries
Lacerations involving the collecting system
|
CT Findings
|
· Suspicion of a collecting system injury should be
raised if free fluid is seen around the kidney on the
initial scan.
· On delayed images contrast-opacified urine is seen
leaking from the collecting system into the
perinephric space.
|
|
Management
|
· The majority of collecting system injuries resolve
spontaneously and do not require intervention.
· Persistent leaks may require insertion of
nephrostomies or JJ ureteric stents to allow healing
of the urothelium.
· Occasionally surgical repair may be needed.
· Urinomas can develop and may require drainage if
they fail to resolve or become infected.
|
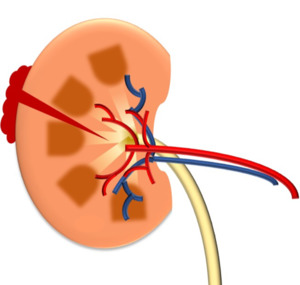
Fig. 8: Illustration of Grade IV laceration involving the collecting system.
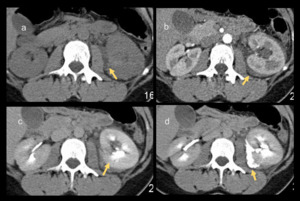
Fig. 9: This case of a 39 year old female involved in a RTA demonstrates the importance of delayed phase imaging in evaluating the collecting system. On the initial non-contrast (a) and corticomedullary phase images (b) free fluid is seen around the left kidney raising the suspicion for a collecting system injury. Delayed (excretory) phase images (c) & (d) show leakage of contrast opacified urine into the perinephric space of the left kidney confirming the injury.
A. Grade V
Shattered Kidney
|
CT Findings
|
· Extensive lacerations involving both renal
parenchyma and the collecting system such that the
kidney is separated into fragments.
· Often devascularised fragments of kidney which are
non-enhancing.
|
|
Management
|
· Usually requires surgical intervention and often
necessitates nephrectomy.
|
Fig. 10: Illustration of shattered kidney.
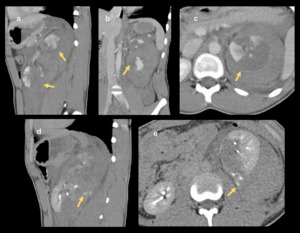
Fig. 11: Shattered kidney in 16 year old male following blunt trauma in a sports match. The left kidney is divided in two (a) & (b). Extensive areas of non-attenuating parenchyma are visible in the upper pole (c) in keeping with devitalised fragments. On delayed phase imaging (d) & (e), extravasation of contrast material from the collecting system of the lower pole can be seen. This patient subsequently underwent left nephrectomy.
Injuries at the renal pedicle
Rapid deceleration injuries such as those sustained in RTAs or following a fall from a height can cause injury at the renal pedicle.
These can involve either the vascular structures,
the pelvicoureteric junction (PUJ) or both.
PUJ Injury
In cases of rapid deceleration the ureter can be stretched and damaged at its proximal fixation point - the PUJ.
This injury can involve either a partial tear or complete avulsion.
Delayed phase imaging is crucial to evaluate these injuries.
|
CT Findings
|
· Extravasation of contrast into the perinephric space
medially on delayed phase images.
· Examining the distal ureter will help distinguish between
a partial tear and complete avulsion:
o Partial Tear: contrast will be seen to opacify the
ureters distally
o Avulsion: No contrast seen in ureters distally
· There may be associated hydronephrosis in the affected
kidney.
|
|
Management
|
· Distinction between partial tear and avulsion important in
determining management strategy:
o Partial Tear: can be managed conservatively with
stenting or urinary diversion with
nephrostomy to allow healing of the
urothelium.
o Avulsion: requires surgical repair.
|
Fig. 12: Illustration showing PUJ avulsion
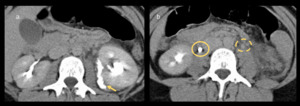
Fig. 13: A 24 year old man following a fall from a height. (a) There is extravasation of opacified urine around the medial portion of the left kidney suggesting damage to the PUJ. (b) There is no contrast within the distal left ureter (dashed circle) unlike the right which is opacified (solid circle), confirming a complete avulsion at the left PUJ.
Vascular Injuries at the renal pedicle
Renal Artery Injury
Shearing forces cause stretching of the renal artery at the pedicle which can result in an intimal tear or dissection.
This in turn promotes thrombosis at the site which can cause occlusion of the vessel.
|
CT Findings
|
· Unenhanced kidney
· Site of occlusion may be visible on maximum intensity
projections.
· Large perinephric haemorrhage with evidence of active
extravasation in cases of laceration or avulsion.
· Retrograde filling of ipsilateral renal vein from the
IVC is suggestive of renal artery injury [10,11].
· There may be peripheral enhancement of the kidney,
the
‘cortical rim sign’ due to collateral supply from capsular,
peripelvic and periureteric branches.
However,
this is a
late finding (>8 hours post injury) and may not be seen
in the acute setting [10].
|
|
Management
|
· Stenting may be performed in cases of arterial occlusion.
· Surgical repair is often required
· Partial/total nephrectomy may be necessary where there
are devitalised fragments.
|
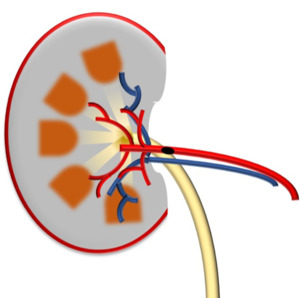
Fig. 14: Illustration of renal artery thrombosis with devascularisation of the kidney.
Renal vein Injury
Renal vein injury is uncommon and it rarely occurs in isolation but is usually associated with injury to either the artery or PUJ.
|
CT Findings
|
· In renal vein thrombosis the vein is enlarged.
There can
be associated nephromegaly,
interstitial oedema and
delayed excretion of contrast into the collecting system.
· Lacerations of the renal vein are not reliably identified
on CT but should be suspected where there is a large
perinephric haematoma [10].
|
|
Management
|
· In cases of isolated renal vein thrombus,
a conservative
approach with anticoagulation is usually preferred.
· Extravasation from a lacerated renal vein may
tamponade and in such cases conservative management
can be employed.
· In cases of haemodynamic instability urgent surgical
repair or nephrectomy may be required.
|
Injuries not covered by AAST grading:
The AAST grading system was developed based on appearances at surgery.
While for the most part it can also be used to classify radiological findings,
some CT findings are not specifically covered:
Active bleeding
|
CT Findings
|
· Irregular linear or flame shaped areas of high attenuation
within a larger area of free fluid.
· On the delayed phase images the area of high attenuation
will have increased in size indicating ongoing
haemorrhage.
|
|
Management
|
· Arterial embolisation can be used in cases of active
arterial bleeding.
· In cases of haemodynamic instability nephrectomy may
be necessary.
|
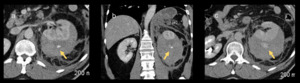
Fig. 15: A small focus of high attenuation in a left perinephric haematoma (a) and (b) is seen to have increased in size on the delayed images (c) indicating active haemorrhage.
Pseudoaneurysm
|
CT Findings
|
· Rounded or oval area which follows the enhancement
pattern of the aorta with high attenuation during the
arterial phase and washout on delayed phase images.
|
|
Management
|
· Arterial embolisation
|
Segmental Renal infarctions
|
CT Findings
|
· Well defined,
wedge shaped areas of low attenuation.
· Base of the wedge at the periphery of the kidney
with apex pointing towards the renal hilum.
· No post contrast enhancement
· Often involving the poles
|
|
Management
|
· Most heal spontaneously and are managed
conservatively
· If they involve >50% of the renal parenchyma
surgical debridement may be necessary to prevent
abscess formation.
|
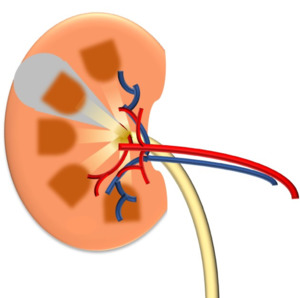
Fig. 16: Illustration of segmental infarct.
Other abdominal injury
Renal trauma rarely occurs in isolation as,
relative to other abdominal viscera,
the kidneys are well protected.
It is vital that the radiologist fully assess all injuries.
The liver is commonly injured in cases of both blunt and penetrating trauma.
Where the mechanism of action involves rapid deceleration,
other relatively mobile structures such as the aorta can be injured.
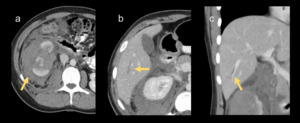
Fig. 17: 18 year old girl kicked by a horse in her right flank. In addition to the renal injury – shattered right kidney (a) a linear area of low attenuation is seen in the liver (b) & (c) consistent with a liver laceration.
Role of Interventional Radiology
The role of radiology in renal trauma is not limited to diagnosis of injury.
With the trend in management of renal trauma moving away from surgical exploration,
minimally invasive techniques are proving more important.
Interventional Radiology can be of benefit in:
- Arterial embolisation for active bleeding or pseudoaneurysms.
- Ureteric stenting or percutaneous nephrostomy to facilitate urothelial healing.
- Drainage of infected urinomas.



 Illustration of renal contusion. (b) 43 year old male post assault. CT shows an ill-defined area of low attenuation in the left kidney consistent with a renal contusion (Grade I injury).")
 Illustration of a subcapsular haematoma. (b) & (c) In this 37 year old woman post blunt trauma, a subcapsular haematoma is seen as a well encapsulated area of low attenuation along the lateral border of the left kidney.")
 grade II and (b) grade III lacerations.")
 & (b).")

 indicating it is an acute haematoma.")
 and corticomedullary phase images (b) free fluid is seen around the left kidney raising the suspicion for a collecting system injury. Delayed (excretory) phase images (c) & (d) show leakage of contrast opacified urine into the perinephric space of the left kidney confirming the injury.")


 & (b). Extensive areas of non-attenuating parenchyma are visible in the upper pole (c) in keeping with devitalised fragments. On delayed phase imaging (d) & (e), extravasation of contrast material from the collecting system of the lower pole can be seen. This patient subsequently underwent left nephrectomy.")

 There is extravasation of opacified urine around the medial portion of the left kidney suggesting damage to the PUJ. (b) There is no contrast within the distal left ureter (dashed circle) unlike the right which is opacified (solid circle), confirming a complete avulsion at the left PUJ.")

 and (b) is seen to have increased in size on the delayed images (c) indicating active haemorrhage.")

 a linear area of low attenuation is seen in the liver (b) & (c) consistent with a liver laceration.")