ECR 2018 / C-2146
Unilateral pulmonary oedema, a forgotten presentation.
Congress:
ECR 2018
Poster Number:
C-2146
Type:
Educational Exhibit
Keywords:
Computer Applications-Detection, diagnosis, CT, Thorax, Lung, Cardiac, Oedema
Authors:
C. A. Arboleda Vallejo1, M. I. carvajal2, M. Perez1; 1Medellin, Antioquia/CO, 2medellin/CO
DOI:
10.1594/ecr2018/C-2146

Fig. 2:
Chest X-ray: Bilateral alveolar opacities of right predominance

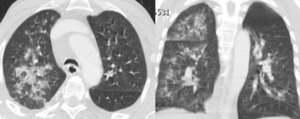
Fig. 3:
Thorax angioTC: Negative study for PE, alveolar opacities in both predominantly...

Fig. 4:
Chest X-ray: control after 2 days, improvement of parenchymal opacities.

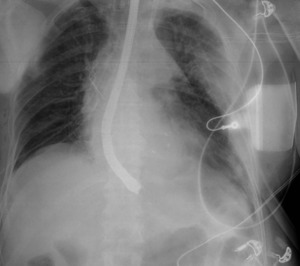
Fig. 5:
Chest X-ray: Bilateral alveolar opacities of right predominance -
...

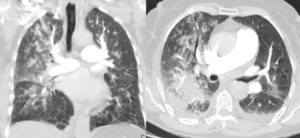
Fig. 6:
Thoracic tomography: Central alveolar occupation with predominance in the right...

Fig. 7:
Chest x-ray: 3 days later, improvement of parenchymal opacities with respect to...

Fig. 8:
Chest x-ray: Mixed bilateral opacities of right predominance - cardiomegaly

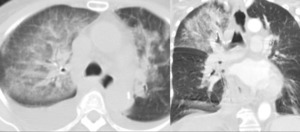
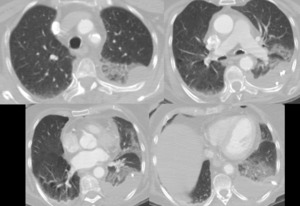
Fig. 9:
Chest tomography: Alveolar occupation of right hemitorax with septal thickening.

Fig. 10:
Control chest radiography: improvement of parenchymal involvement when compared...

Fig. 11:
Chest x-ray: bilateral pleural effusion, the left in abundant amount

Fig. 12:
Chest tomography: Cardiomegaly - Pericardial effusion - Bilateral pleural...