Definition,
prevalence,
etiology and complications
Intussusception is one of the leading causes of acute abdomen in childhood,
and it is a medical emergency that requires prompt diagnosis and management.
It is defined as the invagination of a portion of the proximal bowel (intussusceptum) into a contiguous segment of the distal bowel (intussuscipiens).
Both small and large bowel can be involved,
but ileocolic intussusceptions represent the majority of cases,
more than 80%,
with the terminal ileum acting as the intussusceptum and the ascending colon as the intussuscipiens.
Ileoileocolic,
ileoileal and colocolic intussusceptions are other types of intussusceptions that can also be seen.
(Fig.1)
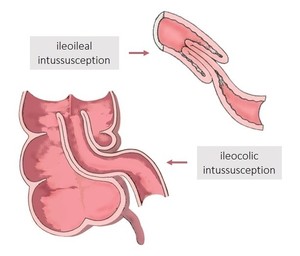
Fig. 1: Ileocolic and ileoileal intussusceptions, schematic drawing.
Intussusception occurs in children of all ages; however it typical presents between 3 to 24 months of age.
It has a male predominance,
with a male:female ratio of approximately 2:1.
The incidence of intussusception varies from 0,66-2,24 per 1000 children in Europe.
This condition has a classical presentation,
with a palpable abdominal mass,
intermittent abdominal pain,
vomiting and “currant jelly” stools,
consisting of blood and mucus mixed with stool,
but these symptoms are seen in less than 50% of patients at the time of presentation.
There is also significant symptomatic overlap with other acute abdominal conditions.
The majority of intussusceptions are idiopathic,
although any condition that produces pathological lead points (lesions in the bowel) can cause intussusception.
Some of these idiopathic cases might be prompted by hyperplastic lymphoid tissue,
implicating a viral or bacterial origin for most cases and acting as the lead point in the distal small bowel.
(Fig.
2)
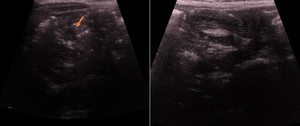
Fig. 2: Ultrasound images with characteristic findings of ileocolic intussusception with lymph nodes (arrow), presumably acting as lead point.
Lead points are typically seen in older children,
including Meckel’s diverticulum,
Henoch-Schönlein purpura,
enteric duplication cyst,
polyp,
bowel wall tumors and lymphoma.
The most common lead point in children older than 5 years is lymphoma and in infants,
the most common is a Meckel diverticulum.
Iatrogenic intussusception has also been described.
If untreated,
intussusception can result in ischemia,
eventually leading to bowel necrosis,
perforation,
peritonitis or even death.
However,
the mortality rate of intussusception is low,
about 2.1 per 1 million live births,
due to the safety and efficacy of current treatments.
Diagnosis
The diagnosis of intussusception is challenging due to its nonspecific symptoms and because young infants often cannot communicate and describe their complaints.
However,
the diagnosis of this condition has been well described and can be established with a high degree of accuracy.
1) Abdominal Radiography
Abdominal radiography may demonstrate an elongated soft tissue mass (typically in the upper right quadrant) with signs of bowel obstruction proximal to it.
A paucity of gas within the right abdomen can also be seen.
The sensitivity of radiography for detection of intussusception is low (about 45%),
however abdominal radiography has an important role in order to exclude pneumoperitoneum prior to reduction.
2) Fluoroscopy
Historically,
an enema with barium,
air,
or water-soluble contrast used to be the standard diagnostic test for intussusception.
Introducing contrast material in the colon demonstrates the leading edge of the intussusception as an intraluminal round or crescent filling defect – meniscus sign.
(Fig.
3)
This diagnostic technique allows the diagnosis of the intussusception and sometimes can be converted to a therapeutic procedure,
enabling reduction of the invagination.
Nevertheless,
fluoroscopy is an invasive technique that has low sensitivity for small-bowel intussusceptions,
provides limited information concerning other causes of acute abdominal pain and involves the exposure to ionizing radiation.

Fig. 3: Water-soluble contrast enema of a ileocolic intussusception. The leading edge of the intussusception appears as an intraluminal round or crescent filling defect – meniscus sign (arrows).
3) Ultrasonography
Ultrasonography (US) has been widely adopted as the first-line modality for the diagnosis of intussusception.
It provides high sensitivity (97,9%) and specificity (99,7%) for detection of this disorder,
allows pathology characterization,
gives information about other causes of acute abdominal pain and can have an important role in guiding treatment. It also doesn’t involve the use of ionizing radiation and is therefore well suited to pediatric patients imaging.
The ultrasound appearance of ileocolic intussusception is characteristic and its typical signs include:
- The target sign or doughnut sign (transverse view): a mass with alternating rings of hyper- and hypoechogenicity.
The hyperechogenic bands are formed by mucosa and muscularis,
whereas the submucosa is responsible for the hypoechoic bands.
(Fig.
4)
- Pseudokidney sign (longitudinal view): it resembles a kidney and consists of bowel wall surrounding hyperechoic mesenteric fat contained within the intussusception.
(Fig.
5)
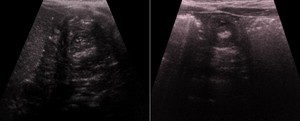
Fig. 4: Transverse ultrasound images showing a swirled pattern of alternating hyperechogenicity and hypoechogenicity - ileocolic intussusceptions. This represents the alternating layers of mucosa, muscularis, and serosa seen in intussusception, giving it a 'target' appearance.
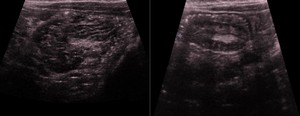
Fig. 5: Longitudinal ultrasound images showing ileocolic intussusceptions with the pseudokidney sign of intussusception, which mimics a kidney. The "renal hilum" is formed by the mesentery's fat and vessels, whereas the "renal parenchyma" is formed by edematous bowel.
The presence of lymph nodes within the lesion’s lumen is a highly suggestive US finding of intussusception and might help distinguish between true intussusception and conditions with a similar presentation.
(Fig.
2)
Ileoileal intussusceptions do not contain lymph nodes,
usually are smaller than 2 cm in diameter and are often transient,
while symptomatic ileocolic intussusceptions typically persist and measure about 2-4 cm.
In intussusception,
the use of US Doppler is important as it helps to guide appropriate management of this situation.
The absence of blood flow within the intussusception is a known predictor of unsuccessful enema reduction and is correlated with complications such as bowel ischemia and necrosis during surgery.
Treatment
Once ileocolic intussusception is confirmed,
doctors recommend the use of enema as initial treatment.
This technique involves instilling air,
saline solution or contrast into the colon,
via the rectum,
with some pressure that reduces the intussusceptum into its normal position,
under real-time imaging observation.
Contraindications for attempting pressure reduction of intussusception include peritonitis and perforation.
US and fluoroscopy can guide the procedure and monitor the reduction.
However,
US has been increasingly used,
with very good success rates while avoiding radiation exposure.
It also may provide a characterization of possible pathological lead points.
Nowadays,
hydrostatic and pneumatic enema are the dominant techniques and are associated with low perforation rates.
Barium has subsequently become less popular because of concerns over peritoneal staining in the event of perforation.
With a hydrostatic enema,
a rectal tube is taped firmly in place and saline solution is introduced slowly by gravity into the rectum.
The hydrostatic pressure usually forces the inverted bowel moves retrograde to the level of the ileocecal valve.
(Fig.
6)
The height of the fluid column is traditionally 3 feet above the patient; further reservoir’s elevation does not significantly alter the intraluminal pressure. The pressure should also be maintained no more than 3 minutes against a non-moving loop intussusception and no more than 3 attempts should be made to reduce an intussusception.
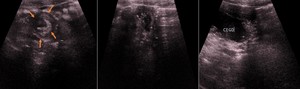
Fig. 6: 1-year old male child presented with classical symptoms of bowel intussusception. Ultrasound shows characteristic findings of ileocolic intussusception – target sign (arrows).
Ultrasound-guided hydrostatic reduction was perfomed with success. Ultrasound images show saline solution within the cecum (CEGO).
In the current method of air reduction,
air is introduced through a rectal catheter,
never exceeding a pressure of 120 mmHg within the colon,
enabling the invagination’s reduction.
When it occurs,
the pressure falls precipitously.
A pressure gauge and popoff mechanism must be present.
It’s important to recognize the findings of US that might reflect an incarcerated intussusception and that may be used to predict the likelihood of a successful enema reduction.
Some of them are:
- small bowel obstruction;
- free intraperitoneal fluid;
- fluid trapped within the intussusception;
- the absence of blood flow within the intussusception.
The success rate of intussusception’s reduction also depends on factors such as the length of time of the intussusception (more than 24 hours),
the degree of the loop and ileocaecal valve’s edema and the presence of lead points.
Normally,
early recurrence is rare,
after a successful enema reduction.
Some indications for surgical treatment are peritonitis,
bowel perforation,
shock and failure of contrast enema.
