
ECR 2018 / C-2480
Pleural pathology – a primer for radiologists
Congress:
ECR 2018
Poster Number:
C-2480
Type:
Educational Exhibit
Keywords:
Lung, Mediastinum, Respiratory system, CT, PET-CT, Digital radiography, Sampling, Diagnostic procedure, Biopsy, Pathology, Cancer, Infection
Authors:
A. Gangahar 1, Z. Wahab1, J. Zhong1, H. Nejadhamzeeigilani1, M. Kon2; 1Leeds/UK, 2Bradford/UK
DOI:
10.1594/ecr2018/C-2480
.
Figure B demonstrates a larger right sided pleural effusion. On both x-rays the hemidiaphragm border of the affected side cannot be delineated.")
Fig. 2:
Chest x-rays showing pleural effusions. On figure A, there is a left sided...
 and lateral (B) chest x-rays demonstrated a loculated pleural effusion in the left oblique fissure.")
Fig. 3:
Frontal (A) and lateral (B) chest x-rays demonstrated a loculated pleural...

Fig. 4:
The patient, a non-smoker, presented with shortness of breath and cough for...
. There is evidence of mediastinal fat invasion (blue arrow) and concern for involvement of the parietal pericardium (yellow arrow). Diagnosis was a right sided mesothelioma.")
Fig. 5:
Contrast enhanced CT shows a large right-sided pleural effusion.
Nodular...
, tracheal shift to the right (arrow) and a depressed left hemidiaphragm.")
Fig. 6:
Chest x-ray showing a left sided tension pneumothorax with a collapsed left...
 showed a right sided pleural effusion with patchy lower lobe consolidation. Pleural aspiration revealed pus and therefore an empyema was diagnosed and a chest drain was inserted (B). Check x-ray (B)showed the drain (arrow) was in the right position. The patient initially improved however 3 days later the patient developed increased shortness of breath and repeat chest x-ray (C) showed a developing lucency in the right hemithorax (arrow). This was initially thought to be a giant bulla however further repeat x-ray (D) showed this may be a loculated pneumothorax (visceral pleura edge seen). The patient proceeded for a CT - see figure 8.")
Fig. 7:
Patient presented with symptoms suggestive of chest sepsis. Chest x-ray (A)...
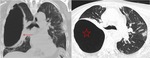
Fig. 8:
Subsequent CT examination (coronal and axial images) confirmed an encysted...
 showing bilateral calcified structures (arrows), some of which have incomplete borders. Axial CT (B and C) reveal these to be calcified pleural plaques (arrows).
Pearl: Mediastinal pleural involvement is an concerning feature of an malignant cause.")
Fig. 9:
Chest x-ray (A) showing bilateral calcified structures (arrows), some of which...

Fig. 10:
Axial contrast enhanced CT showing a pleurally based soft tissue lesion with...
 showing left sided pleural mass with obtuse borders (arrow). Axial CT (B and C) reveal this to be of fat density (arrows) in keeping with a pleural lipoma. Pitfall: Use appropriate windowing to find fat density pleural abnormalities that may be missed on soft tissue windows.")
Fig. 11:
Chest x-ray (A) showing left sided pleural mass with obtuse borders (arrow)....
 showing left sided pleural lesion with obtuse borders (arrow). Axial CT (B) reveals this to be of fat density (arrows) in keeping with a pleural lipoma. Further extension of this fatty lesion out of thorax into the chest wall soft tissue and displacing the overlying chest wall muscles.")
Fig. 12:
Chest x-ray (A) showing left sided pleural lesion with obtuse borders (arrow)....
 showing left sided circumferential pleural thickening (arrows) and blunting of the left costophrenic angle. Axial CT (B and C) reveals this to be circumferential pleural thickening with enhancement (arrows) with intra-pleural cystic loculations/septae concerning for empyema. Left sided pleural fluid also noted. Pleural biopsy confirmed tuberculosis.")
Fig. 13:
Chest x-ray (A) showing left sided circumferential pleural thickening (arrows)...
 showing bilateral perihilar opacities, particularly in the right upper zone (arrows) and thicker linear opacities in the right mid-zone (blue arrow).
Axial high resolution CT (B and C) shows bilateral perilymphatic, subpleural and fissural nodules (arrow on B). The have coalesced and formed larger linear opacities in keeping with sarcoid granulomas (arrow on C). Evidence of pleural nodularity. There was also evidence of bilateral hilar lymphadenopathy. Imaging features in keeping with pulmonary and pleural sarcoid.")
Fig. 14:
Chest x-ray (A) showing bilateral perihilar opacities, particularly in the...
 which is shifted towards the right of the midline (dotted line).")
Fig. 15:
Patient with previous TB and empyema. Chest x-ray showed dense calcifications...
 show circumferentially thickened and nodular pleura (arrows) which enhances and involves the mediastinal surface and invades the mediastinal fat. Biopsy confirmed malignant mesothelioma.")
Fig. 16:
Contrast enhanced axial CT images (A and B) show circumferentially thickened...

Fig. 17:
CT thorax images from the same patient showing multiple pleural deposits,...

Fig. 18:
Patient with a history of self-neglect was admitted with shortness of...
 showed the patient had developed a tension pneumothorax with complete collapse of the right lung and evidence of midline shift towards the left side (arrows). A chest drain was inserted and the patient was stabilised. Post chest drain x-ray (b) 2 days later shows partial re-expansion of the lung, a residual hydropneumothorax and a cavitating lesion in the right upper lobe (arrow). Due to respiratory failure, the patient required intubation and admitting to the Intensive Care Unit.")
Fig. 19:
During admission, the patient deteriorated and shortness of breath acutely...
 shows a large right sided hydropneumothorax and cavitating lung lesions (arrow) with dense consolidation and lung collapse (star).
Coronal image (b) highlighted the numerous cavitating right lung lesions and extent of the confluent consolidation. Further ground glass infective change (green arrow) in the left lung also present.
Evidence of loculated right pleural fluid in keeping with infection and empyema formation. The aspirate grew Staphylococcus Aureus species.")
Fig. 20:
CT thorax was undertaken for further assessment. The axial image (a) shows a...
 reveal a right sided empyema (arrow) with pleural enhancement. 2 chest drains in-situ on the right. The lung window images (b and c) show the extensive multiloculated lung abscesses in fistulous communication (arrows) with the bronchial tree and therefore confirming a bronchopleural fistula.")
Fig. 21:
Despite conservative management the patient did not improve and repeat CT...