Complications in LAGB
In patients with LAGB,
UGS can identify various abnormalities connected with the gastric banding system (rotation,
dislocation,
rupture of the band,
breakage of the subcutaneous port or of the connection tube) and organic damages such as gastric stenosis,
prolapse,
and gastric wall erosion.
In fig.
4 we present some cases in which the connection tube between the port and the gastic band is interrupted (connection tube breakage or disconnection).
This can be subsequent to a trauma or can be spontaneous.
The main result from this complication is the regain of weight because the band cannot be inflated with saline solution,
which escapes from the system.
In these cases,
with a simple plain preliminary film the radiologist is able to easily confirm the clinical suspiction.
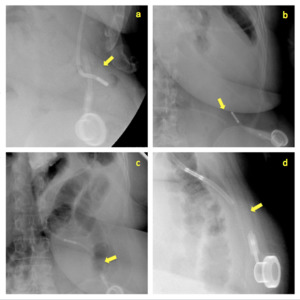
Fig. 4: Different cases of connection tube breakage or disconnection (arrows).
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
In more difficoult cases,
to identify breaking point,
can be useful to perform a diagnostic bandogram injecting some hydrosoluble contrast medium in the system through the subcutaneous port and observing in which point does the contrast medium escapes (fig.
5).

Fig. 5: Bandogram showing hydrosoluble contrast medium leaking from an interrupted connection tube (arrow).
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Tip: if possible,
bandogram should be done before oral contrast administration or,
at least,
by changing projections to avoid overlay images.
Tip: we suggest to follow carefully with continuous fluoroscopy the course of the whole tube and its connections with the band and the port,
asking the patient to rotate his body with very slow movements.
In fig.
6 we describe another very common complication: the rotation of the band,
which can be easily demonstraded by a preliminary plain film; infact,
an alteration of the phi-angle can be seen.
The phi-angle is conventionally the angle mesaured between a vertical line orientated to the vertebral column and another through the long-axis of the gastric band; it normally ranges from 4 to 58 degrees [9].
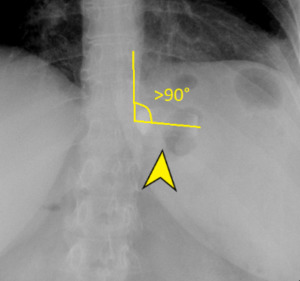
Fig. 6: Gastric band rotated (arrowhead); in this case, phi-angle is > 90°.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Tip: the phi-angle must be measured with the gastric band in profile.
One of the consequences of the rotation of the ring can be the onset of a stricture with the formation of an abnormal gastric fundus pouch.
In these cases,
obstructive sympthoms as nausea,
vomiting and reflux can be observed.
In fig.
7 we demonstrate,
through a dynamic UGS,
a stricture of the neostoma,
due by the band with a dilated gastric pouch in which contrast medium-fluid and air-fluid levels are also present.
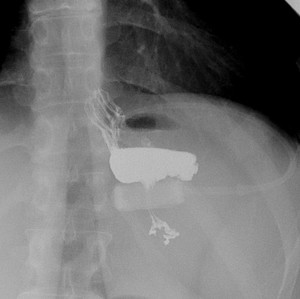
Fig. 7: Gastric stricture caused by a tight, rotated band; in the image are evident the subsequent dilatation of the upstream gastric pouch, the poor contrast medium progression and both a contrast medium-fluid and an air-fluid level.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Tip: in our centre,
a bariatric surgeon is always present at the time of the investigation,
in order to promplty deflate the band through the aspiration of an amount of saline solution from the port,
giving the patient an immediate relief from the symptoms.
The radiologist,
on the other hand,
can help the surgeon to identify the port with real time images,
if the access with the needle is difficult.
Subcutaneous port can be rotated and oriented downwards (fig.
8),
making the puncture for calibration difficoult for the surgeon.
With fluoroscopy,
the radiologist can help in managing the calibration procedure.

Fig. 8: Subcutaneous port displacement (facing downwards).
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
In many cases,
the stricture rises just because the band is calibrated too tight in an attempt to increase weight loss.
A stricture can appear not only when the band is not just tight,
but also when there is a dislocation of the gastric band, with leads to a sort of stomach throttling.
The contrast medium swallow cannot go beyond the ring and tends to accumulate upstream in a gastric fundus pouch,
which ofter appears dilated.
When a part of stomach below the ring tends to go up through the band,
in some cases reaching the thorax,
there is a gastric prolapse,
which is the most common complication of LAGB necessitating reoperation (fig.
9).
Major casuses of band dsilocations and subsequent possible gastric prolapse might be improper surgical fixation,
premature reintroduction of solid food and recurrent vomiting.
In most severe cases,
gastric prolapse can lead to gastric necrosis,
obstruction,
esophageal or gastric dilatation with perforation,
malnutrition,
and dehydration [10].

Fig. 9: Gastric prolapse; the gastric band is tight, dislocated and rotated. The portion of stomach upstream the ring is dilated and with its major axis rotated anteriorly.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
In fig.
10 an other serious complication is shown: a gastric wall erosion. In this situation, the band erodes the gastric wall around it and moves further into the gastric lumen.
The administration of oral contrast medium,
which in this case pools around the band,
gives the radiological confirmation of the erosion.
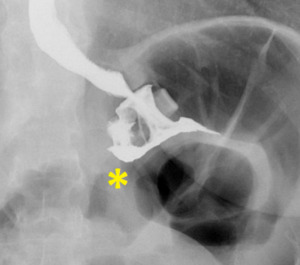
Fig. 10: Gastric wall erosion (asterisk underlines a small amount of contrast medium passage outside the ring).
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Tip: in our clinical practice,
patients with this complication present typically some years after LAGB placement with chronic epigastic pain associated to a no more satisfying weight loss.
A gastric wall erosion is always to be suspected when the ring seems dislocated.
There are some more rare cases of LABG complications been described in literature,
as a cases of early perforation of the gastric band device,
diagnosed through a bandogram [11] and other some more rare cases of band breakage or opening [12].
Complication in LSG
In LSG,
complications can be divided into early and late.
Early complications: in the earliest follow-up major findings are leaks and fistulae,
invariably due to an anastomotic dehiscence along the suture line (fig 11 a,
b).
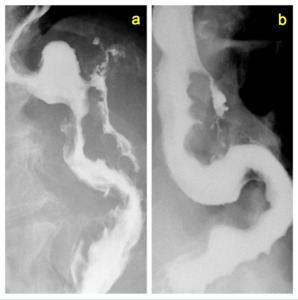
Fig. 11: Two different cases of an early staple-line dehiscence after LSG, leading to an extra-gastric leak of contrast medium.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Tip: clinical examination is important: the onset of these complications is often accompanied by signs of inflammation as fever,
acute abdominal pain and leukocytosis.
Tip: the UGS must be done not only in frontal,
but also in lateral and oblique projections to well determine the anatomic origin of the leak and its morphology.
If a drainage tube is present,
it is possible to observe its intraluminal opacification with extravasated contrast medium.
To complete the diagnosis and to search for infected collections,
an abdominal CT scan is mandatory.
In our centre,
leaks and fistulae are treated at first with a radiological percutaneous approach. The possible radiologic treatments include: drainage of the abdominal collection,
positioning of drainage in the fistula,
embolization of the leak with a synthetic biodegradable cyanoacrylate basis glue.
Our most recent study demonstrated theat these procedures were effective in 68% of the cases.
Late complications: Possible findings in the late follow-up are strictures of the gastric tubule,
causing a transit slowdown associated with episodes of recurrent nausea, vomiting and with general sickness (fig.
12 a,
b).
Strictures may be due to to operative technique (adhesions) but also to healed previous leaks and fistulas.
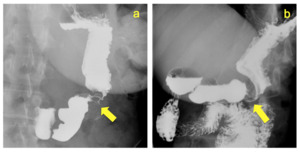
Fig. 12: Two different cases of stricture (arrows) of the gastric tubule, with a slowdown of contrast medium passage.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Tip: Strictures can be easily identified with a dynamic UGS with multiplanar projections.
They can be treated with endoscopic balloon dilatation sessions or with the placement of a metal stent.
UGS are useful to follow-up the patients after dilatation sessions, to check the stent patency as well as to check possible stent dislocations or leaks (as in fig.
13).
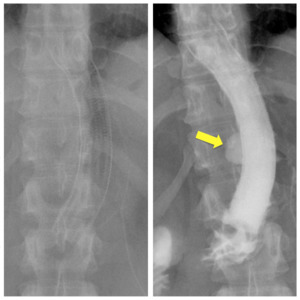
Fig. 13: Radiographs showing a correctly positioned metallic stent, placed to expand a gastric remnant stricture after LSG (left); a control examination, some days later, demonstrates a further complication: a leakage of contrast medium through the wall of the stent (right).
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Another late complication can be the herniation of part of the gastric remnant through the diaphragmatic hiatus; symptoms may include epigastric or chest pain,
postprandial fullness,
nausea and vomiting.
The causes are similar to those related to herniation after LAGB,
in particular recurrent vomiting is a favoring factor. The case below (fig.
14) shows the cranial part of the gastric tubule largely herniated in the thoracic region.
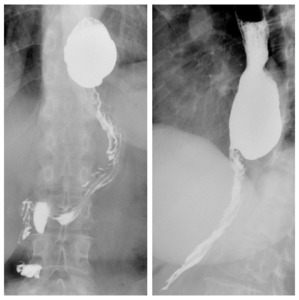
Fig. 14: Large hiatal hernia of part of the gastric remnant after LSG; frontal (left) and left oblique view (right).
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
An other chronic condition is and long-term gastric remnant re-dilatation (fig.
15).
The dilatation can be partial and in this case the gastric fundus remnant dilatation is more frequent,
or complete,
when the whole stomach remnant gets larger.

Fig. 15: Gastric remnant dilatation 3 years after LSG. The volume of the remnant, through tridimensional software reconstructions, was been estimated significantly higher than in the immediate postoperative period.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
It has been demonstrated, in one of our recent studies,
that there is a significant volumetric increase of the gastric tubule in the six years following the intervention,
as measured by UGS; despite this,
we demonstrated,
in long-term follow-up,
that re-dilatation does not seem to affect the weight loss.
Complications in RYGB
RYGB's most frequent complications are anastomotic dehiscence,
with extraluminal leak of contast medium,
and anastomotic strictures,
with slow or stuck contrast medium transit,
frequently due to technical causes or conditioned by tissue repair.
There are some other more rare anatomical modifications,
with subsequent altered clinical conditions,
strictly related to the surgical technique,
as the onset of a “candy-cane” syndrome.
This is caused by an excessive lenght of nonfunctional Roux limb proximal to the gastrojejunostomy, which becomes redundant and turns into a sort of tank in which food and liquids are incarcerated (fig.
16); infact while doing an UGS an air-fluid level is often observable.
This name was assigned because of the shape of the redundant limb,
appearing similar to a candy stick.
Tip: this condition can lead to symptoms such as nausea,
food regurgitation,
vomiting,
reflux and epigastric pain.
Radiologist must always search for a "candy cane" limb in presence of these disorders after RYGB.
Tip: if the afferent limb is early and preferentially with respect to the efferent loop injected with contrast medium,
a "candy cane syndrome" is to suspect. UGS are necessary to confirm it and to demonstrate the morphology,
the length and the course of the abnormal Roux limb,
allowing a re-intervention planning.
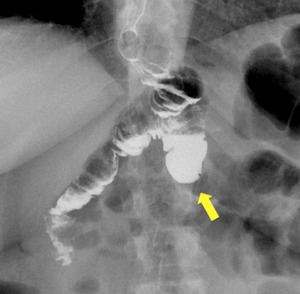
Fig. 16: Frontal view of a blind afferent jejunal limb with an excessive length (arrow), leading to a "candy cane syndrome" in a patient with gastro-jejunal anastomosis in RYGB.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
The surgical resection of the aberrant limb is recognized as effective therapeutic option to completely avoid symptoms.
In one patient,
we identified a rare case of herniation of the gastric pouch in the thoracic region,
causing severe reflux symphoms (fig.
17).
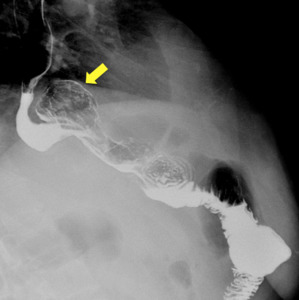
Fig. 17: RYGB complicated with the herniation of the gastric pouch in the thoracic region through the diaphragm (arrow); right oblique view.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Some authors described,
in bariatric surgery,
as well in oncologic surgery,
the possible onset of an internial hernia after gastric bypass [13].
Tip: diagnosis of an internial hernia is quite difficoult with UGS; it must be confirmed with other radiological examinations,
as a CT scan.
General complications after bariatric surgery: there are some complications which are common to every type of bariatric intervention; for this reason,
they cannot be assigned to one precise type of procedure.
Motility disorders as gastroesophageal reflux,
usually accompanied by disfuncional oesophageal waves,
i.e.
tertiary waves (fig.
18) are frequently diagnosed after gastro-intestinal surgery,
including bariatric surgery.
The symptoms are typical and are heartburn,
gastric acidity,
precordial pain,
regurgitation,
nausea and in some cases,
vomiting.

Fig. 18: Motility alteration in a LSG patient developing severe gastro-esophageal reflux up to the proximal esophagus, accompanied by tertiary waves.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Tip: the study of spontaneous gastroesophageal reflux is simple for the fact that it is possible,
just with a fluoscopic observation,
to underline the retrograde movement of the contrast medium from the stomach,
the gastric remnant or the digiunal anastomized limb.
Some patients can complaint reflux during nighttime or when they are in a supine or outstretched position.
For this reason,
the radiologist must search for gastroesophageal refux also through provocative maneveurs in the supine position,
asking the patient to cough or asking to do a straining manouvre.
After bariatric surgery,
it is also possible to observe some anatomical modifications in neighboring organs,
as the onset of a postsurgical epiphrenic diverticulum, which is a pulsion diverticulum of the distal oesophagus arising just above the lower oesophageal sphincter (fig.
19).

Fig. 19: Onset of an epiphrenic diverticulum (arrow) protruding from the left distal esophageal wall in a patient undergoing LSG.
References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT
Tip: in this latter case,
oblique projections are indicated to describe the dimensions and the morphology of the diverticulum in anticipation of a possible surgical resection.

. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")
. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")
; in this case, phi-angle is > 90°. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")

. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")

. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")

 of the gastric tubule, with a slowdown of contrast medium passage. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")
; a control examination, some days later, demonstrates a further complication: a leakage of contrast medium through the wall of the stent (right). References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")
 and left oblique view (right). References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")

, leading to a "candy cane syndrome" in a patient with gastro-jejunal anastomosis in RYGB. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")
; right oblique view. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")

 protruding from the left distal esophageal wall in a patient undergoing LSG. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")