ECR 2018 / C-2603
Biliary anastomotic strictures in liver transplantation: outcomes of percutaneous treatment
Congress:
ECR 2018
Poster Number:
C-2603
Type:
Scientific Exhibit
Keywords:
Interventional non-vascular, Biliary Tract / Gallbladder, Liver, Percutaneous, Fluoroscopy, Dilation, Stents, Laboratory tests, Transplantation, Dilatation
Authors:
A. Bertesso, G. Barbiero, M. Battistel, D. Miotto; Padova/IT
DOI:
10.1594/ecr2018/C-2603

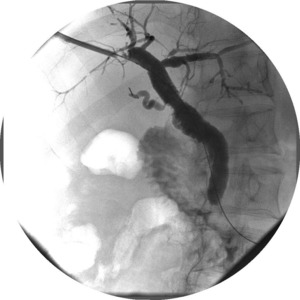
Fig. 1:
Cholangiographic control shows primary patency after balloon dilatation.

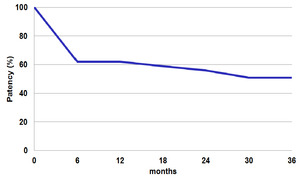
Table 1:
Kaplan-Meier chart showing primary success in the management of patients with...
. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")
Fig. 2:
Cholangiographic restoration of patency with rapid contrast medium transit...

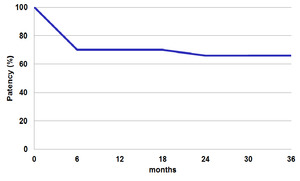
Table 2:
Kaplan-Meier chart showing primary or secondary success in the management of...

Fig. 3:
Cholangiographic control of bare metal stent, correctly positioned.

Fig. 4:
Cholangiographic control of bare metal stent with rapid contrast medium transit...
. References: U.O.C. Radiologia Universitaria, Università degli Studi di Padova, Azienda Ospedaliera di Padova - Padova/IT")
Fig. 5:
Cholangiographic control of bare metal stent with incomplete contrast medium...

Fig. 6:
Percutaneous cholangiographic control in patient with stenosis' dilatation...

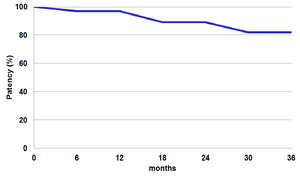
Table 3:
Kaplan-Meier curve shows that the percentage of patients treated with success...

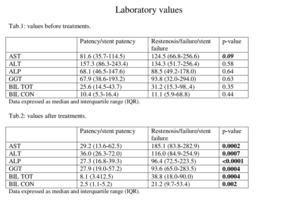
Table 4:
Comparison charts of laboratory values before and after the treatment.