Type:
Educational Exhibit
Keywords:
Haemorrhage, Dementia, Education, Diagnostic procedure, CT, MR, Vascular, Neuroradiology brain
Authors:
L. Quintana Barriga1, R. F. Ocete Pérez1, A. M. Fernández Plaza2, F. Álvarez Jáñez1, M. Avila Macias1, E. fajardo1; 1Sevilla/ES, 2Huelva/ES
DOI:
10.1594/ecr2018/C-2742
Background
Cerebral amyloid angiopathy (CAA) is a common condition,
usually sporadic,
present in 10-40% of elderly brains and its prevalence can be higher than 80% in Alzheimer disease (AD).
CAA is responsible for 10-20% of lobar intracerebral haemorrhages (ICH) and it is considered the most frequent non-traumatic cause of ICH in non-hypertensive patients [1].
CAA is a cerebrovascular disorder caused by deposition of amyloid-β protein in the tunica media and adventitia of cerebral blood vessels,
especially in both medium- and small-sized.
This leads to a vascular fragility that may cause lobar haemorrhage (both micro- and macro-),
small ischemic events and leukoencephalopathy [2].
Microbleeds secondary to amyloid microangiopathy are usually punctate,
very numerous,
and their most frequent locations are the cortical and cortical-subcortical areas (Fig. 1).
Diagnosis of CAA is based on the modified Boston criteria (Table 1)[3].
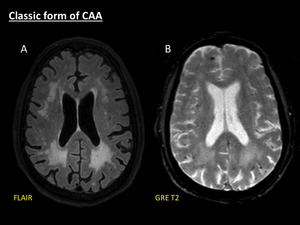
Fig. 1: Classic form of CAA. Axial fat-suppressed FLAIR (A) shows patchy symmetrical white matter hyperintensities without mass effect, with periventricular confluence, related to Fazekas 3 leukoencephalopathy. Axial GRE T2 (B) demonstrates several microbleeds manifested as multiple punctate hypointensities located in cortical and cortical-subcortical areas.
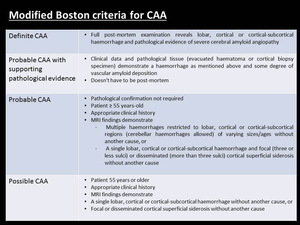
Table 1: Modified Boston Criteria for CAA.
References: van Rooden S et al. Descriptive analysis of the Boston criteria applied to a Dutch-type cerebral amyloid angiopathy population. Stroke. 2009;40(9):3022–7.
Cerebral amyloid angiopathy-related inflammation (CAA-ri) is a recently described uncommon manifestation of CAA,
which is histologically related to cerebral amyloid inflammatory vasculopathy and cerebral amyloid angiitis.
It is clinically manifested as a subacute syndrome of reversible encephalopathy with accelerated cognitive decline,
headache,
behavioural changes,
stroke-like signs and/or seizures,
often with a recurrent presentation [4,
5].
Diagnostic criteria proposed by Chung et al.
are based on neuroimaging and can avoid unnecessary biopsy to confirm the disease (Table 2) [5].
Early diagnosis has a significant impact on patient prognosis as up to three-quarters of the patients with biopsy-proven AAC-ri respond to corticosteroid therapy [6,
7].
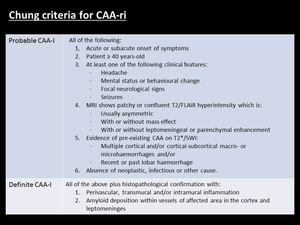
Table 2: Chung criteria for CAA-ri.
References: Chung KK et al. Cerebral amyloid angiopathy related inflammation: Three case reports and a review. J Neurol Neurosurg Psychiatry. 2011;82(1):20–6.

 shows patchy symmetrical white matter hyperintensities without mass effect, with periventricular confluence, related to Fazekas 3 leukoencephalopathy. Axial GRE T2 (B) demonstrates several microbleeds manifested as multiple punctate hypointensities located in cortical and cortical-subcortical areas.")
:3022–7.")
:20–6.")