Liver transplantation (LT) represents the treatment of choice in end-stage liver disease; the main indications [1,
5] are:
- cholestatic diseases: biliary atresia (about 46% of all pediatric LTs),
Alagille syndrome,
sclerosing cholangitis,
Caroli disease,
etc.
- metabolic diseases: maple syrup urine disease,
α1-antitripsin deficiency,
tyrosinemia,
Wilson's disease,
etc.
- liver tumors: hepatoblastoma,
hemangioendothelioma
- acute liver failure (very rare in children).
Surgical techniques [1,
3]:
- whole-LT: performed as in adults,
with classic (inferior vena cava replacement) or piggyback (preservation of the native inferior vena cava) technique;

Fig. 1: Whole-LT in a case of hepatoblastoma.
References: Radiology Unit - Department of Medicine - University Hospital of Padova
- reduced size-LT: the whole liver from an adult cadaver donor is reduced in size,
obtaining a left lateral segment graft (segments 2 and 3) without the vena cava; the remaining liver is discarded;
- living related-LT: the left lateral segment is provided by a healthy donor,
usually a relative; relative size match and compatible blood group are necessary;
- split-LT: two partial organs are obtained by a single liver: the left lateral segment (for pediatric transplant) and the extended right liver (which includes segments 1 and 4-8,
for adult patients);

Fig. 2: A case of left split-LT.
References: Radiology Unit - Department of Medicine - University Hospital of Padova

Fig. 3: A case of right split-LT.
References: Radiology Unit - Department of Medicine - University Hospital of Padova
- auxiliary orthotopic-LT: the left lobe of the recipient is removed and a left lateral segment is placed orthotopically as an auxiliary support.
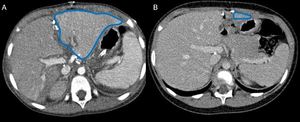
Fig. 4: Acute liver failure treated with liver transplantation using the auxiliary orthotopic split (blue line). CT images, performed immediately after surgery (A) and two years later (B), show progressive left lobe atrophy after immunosuppressive therapy interruption.
References: Radiology Unit - Department of Medicine - University Hospital of Padova
Vascular and biliary anastomoses are performed differently in case of whole-LT and reduced size-LT [4].
In whole-LT:
- the graft's hepatic artery is usually anastomosed in an end-to-end way to the recipient's;
- the main portal vein (MPV) anastomosis is also created in an end-to-end way;
- the inferior vena cava can be reconstructed end-to-end,
both in the suprahepatic and the infrahepatic tract or through the piggyback technique, that implies the recipent's inferior vena cava sparing and subsequent anastomosis to the graft's hepatic veins;
- common bile duct anastomosis is usually performed through a duct-to-duct reconstruction, except in patients with biliary atresia,
in whom a Roux-en-Y hepaticojejunostomy is necessary.
In reduced size-LT:
- in case of discrepancy in size between the graft's and the recipient's hepatic artery,
arterial reconstruction is performed through a donor conduit from the infrarenal aorta;
- portal vein anastomosis is created end-to-end,
usually between the graft's left portal vein and the recipient's MPV;
- the hepatic venous anastomosis is performed through the piggyback technique,
between the graft's left hepatic vein and the recipient's hepatic vein orifice;
- the biliary tree is reconstructed through a Roux-en-Y hepaticojejunostomy.
Post-operative complications are frequent after LT,
in particular in pediatric patients,
due to the different surgical techniques,
used to increase the availiability of potential grafts [1].
The early detection of these complications can lead to a prompt treatment,
avoiding graft failure and subsequent retransplantation.
Even if the most frequent complications are those of biliary origin,
the vascular ones are the most dangerous for the survival of the graft [2,
4,
5].
We reviewed only complications that can be studied with radiological examinations.
Early complications (<30 days):
- biliary: strictures,
leakages,
cystic duct mucocele
- vascular: hepatic artery thrombosis,
portal vein thrombosis,
vascular leakages,
pseudoaneurysm
- others: hematoma,
collections,
abscess,
bowel perforation,
fistulae.
Late complications:
- biliary stenoses,
cystic duct mucocele
- vascular stenoses.




. CT images, performed immediately after surgery (A) and two years later (B), show progressive left lobe atrophy after immunosuppressive therapy interruption. References: Radiology Unit - Department of Medicine - University Hospital of Padova")