ECR 2018 / C-2748
Early and late complications after pediatric liver transplantation: imaging features and percutaneous treatments.
Congress:
ECR 2018
Poster Number:
C-2748
Type:
Educational Exhibit
Keywords:
Transplantation, Diagnostic procedure, Cholangiography, Angioplasty, Percutaneous, MR, CT, Paediatric, Liver, Abdomen
Authors:
A. Cavaliere1, A. Varotto1, S. K. J. Flores Quispe1, C. Dengo2, V. De Lorenzo1, C. Zivelonghi1, M. Zuliani1, T. Toffolutti1, R. Stramare1; 1Padua/IT, 2Padova/IT
DOI:
10.1594/ecr2018/C-2748

Table 1

Table 2

Table 3
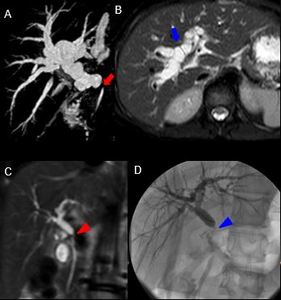
 and an axial T2-weighted SPAIR image (B) showing a duct-to-duct anastomosis stricture (red arrow) associated with intrahepatic bile ducts dilatation (blue arrow), 2 weeks after whole-LT in a 11-year-old girl.
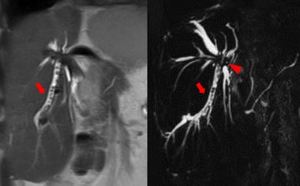
A coronal T2-weighted MR sequence (C) showing the duct-to-duct anastomosis stricture (red arrowhead) 28 days after whole-LT in a 14-year-old girl.
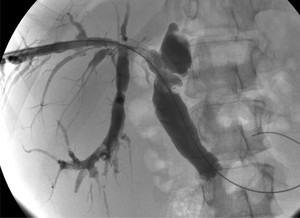
The stricture was confirmed by a percutaneous cholangiography (D), that shows the lack of contrast medium transit through the anastomosis (blue arrowhead). References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 5:
A cholangiography MR sequence (A) and an axial T2-weighted SPAIR image (B)...
 and a cholangiography MR sequence (B), in a 13-year-old boy.
Another case of early cystic duct mucocele, associated with intrahepatic bile duct dilatation in a 2-year-old girl, 10 days after the whole-LT, shown in a T2-weighted image (C) and in the cholangiography MR sequence (D). References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 6:
A case of massive cystic duct mucocele associated with biloma occurred 29 days...
 and biliary stent occlusion, previously positioned for a biliary-jejunal anastomosis stricture (arrowhead). References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 7:
A 18-year-old boy with biliary lithiasis (red arrow) and biliary stent...

Fig. 8:
In the same patient, in-stent restenosis was treated with a percutaneous...

Fig. 9:
Post-procedural cholangiography showing stent patency in the previous patient.
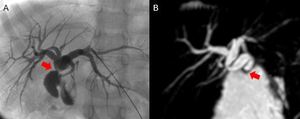
 in a 3-year-old girl 2 years after a whole-LT, shown in percutaneous cholangiography (A) and cholangiography MR (B), with slight intrahepatic bile ducts dilatation. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 10:
Biliary-jejunal anastomosis stricture (red arrow) in a 3-year-old girl 2 years...
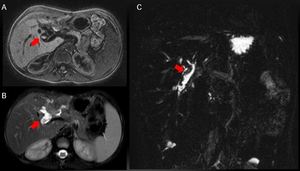
 in a 9-year-old girl with cholestasis 7 months after a right split-LT, demonstrated by axial T1-weighted GE SPIR (A) and T2-weighted SPAIR (B) sequences and cholangiography MR (C). References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 11:
Biliary plugs (red arrows) in a 9-year-old girl with cholestasis 7 months after...

Fig. 12:
Cystic duct mucocele can also occur later. The two cholangiography MR images...
. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 13:
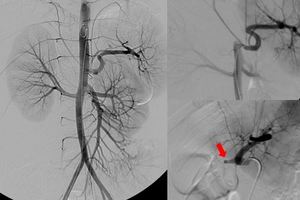
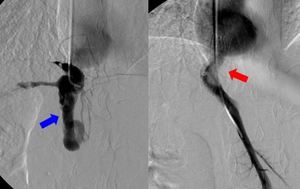
A 9-year-old girl with hepatic artery thrombosis 22 days after right split-LT:...
 hepatic artery thrombosis (red arrowhead) and (B) portal vein thrombosis (red arrow) with diffuse liver hypoperfusion. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 14:
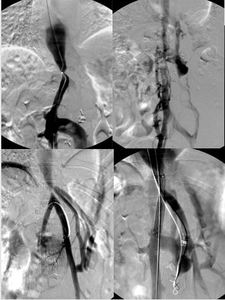
A case of combined vascular complications in a 2-year-old girl 2 days after a...
. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 15:
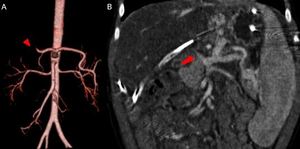
A 2-year-old boy with hepatic artery thrombosis, 11 days after the liver...
. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 16:
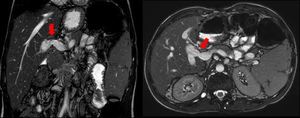
A 18-month-old girl with extrahepatic portal vein thrombosis and subsequent...

Fig. 17:
US imaging of a portal vein anastomotic stenosis developed 6 years after...
, 3 years after the right split-LT, as shown in balanced-SSFP sequences. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 18:
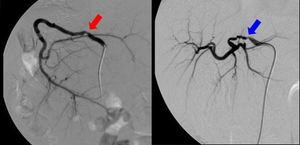
A 12-year-old boy who developed portal vein anastomotic stenosis (red arrows),...
 3 months after left split-LT.
Another 2-year-old girl with 70% hepatic artery anastomotic stenosis (blue arrow) 10 months after whole-LT. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 19:
A 2-year-old girl with 50% hepatic artery anastomotic stenosis (red arrow) 3...
, developed eleven years after the split-liver transplantation and treated with several angioplasties and a stent positioning (red arrow). References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 20:
A 13-year-old boy with hepatic vein stenosis and collateral vessels (blue...

Fig. 21:
A 9-year-old girl with hepatic vein stenosis and collateral vessels, developed...
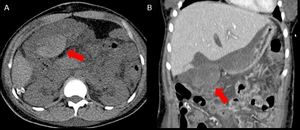
 and after (B) contrast medium injection show a intra-peritoneal perihepatic hematoma (red arrows) occurred 5 days after whole-LT. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 22:
CT images before (A) and after (B) contrast medium injection show a...
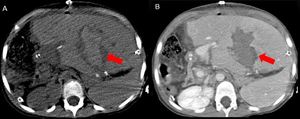
 and after (B) contrast medium injection show an intrahepatic hematoma (red arrows) 2 weeks after left split-LT. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 23:
CT images before (A) and after (B) contrast medium injection show an...
. The surgical re-intervention demonstrated multiple transverse colon perforations. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 24:
CT image, performed 10 days after whole-LT, showing gas bubbles inside the...
 occurred 10 days after whole-LT. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
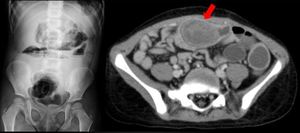
Fig. 25:
A case of perihepatic fluid collection containing gas (red arrow) occurred 10...
 inside the ileum. Surgical intervention demonstrated a bezoar made of contrast medium from multiple previous percutaneous biliary procedures. References: Radiology Unit - Department of Medicine - University Hospital of Padova")
Fig. 26:
A curious case of small bowel subocclusion 3 years after whole-LT:...