Normal arterial vascular anatomy [1]:
The upper limb vasculature originates at the aortic arch and extends through to the digital arteries (Figure 1).

Fig. 1
References: Adapted from: ‘Arteries & veins of the upper limb’, Marc REVOL 2010.
Subclavian artery
-
Arises from the brachiocephalic artery on the right and aortic arch on the left,
running posterior to the subclavian vein and anterior scalene muscles
-
Five main branches: vertebral artery,
internal thoracic artery (internal mammary artery),
thyrocervical trunk,
costocervical trunk,
and dorsal scapular artery
-
Blood supply to head,
neck,
chest and scapula
Axillary artery
-
Continuation of the subclavian artery as it crosses the lateral margin of the first rib
-
Major branches: superior thoracic,
thoracoacromial,
lateral thoracic,
subscapular,
and anterior and posterior humeral circumflex arteries
-
Supplies the shoulder,
humerus,
scapula and chest wall
Brachial artery
-
Continuation of axillary artery after crossing the inferior margin of teres major/posterior axillary fold,
passing medially along the upper arm
-
Major branches: deep brachial artery and smaller arteries around elbow joint including superficial brachial artery
Radial artery
-
Division of brachial artery at the antecubital fossa,
coursing along lateral side of the forearm to the wrist
-
Major branches: recurrent radial artery proximally,
deep palmar arch distally
Ulnar artery
-
Division of brachial artery at the antecubital fossa,
coursing along medial side of the forearm to the wrist
-
Major branches: posterior and anterior recurrent ulnar arteries proximally,
common interosseous artery in upper forearm,
superficial palmar arch distally
Common variant arterial anatomy [2]:
-
High origin of the radial artery from the axillary (2.7 - 5.0%) or upper brachial artery (5.9 - 12.1%)
-
High origin of the ulnar artery is less common (0.17 - 0.2%)
-
Duplicated brachial artery
-
Direct origin of the superficial brachial artery from axillary artery
-
Trifurcated brachial artery (most commonly either radial,
ulnar and anterior recurrent ulnar artery,
or radial,
ulnar and common interosseous artery)
-
Hypoplastic/aplastic radial and ulnar arteries
-
Persistent median artery – lack of regression of the median branch arising from the common interosseous artery (2.0 - 4.0%)
The main types of vascular injury include [3,
4]:
- Intimal injuries
- Complete wall defects – active bleeding and pseudoaneurysm
- Transection
- Arteriovenous fistula
- Contained haematoma
- Vasospasm
Intimal injuries
The innermost layer of the artery,
or intima,
is damaged.
Damage can result in flaps,
disruptions or subintimal/intramural haematomas.
They are more common in the setting of blunt trauma.
Typical CT appearances:
-
Flaps – internal linear filling defects (Figure 2)
-
Disruptions – change in vessel calibre
-
Subintimal or intramural haematoma – intermediate density within a vessel wall
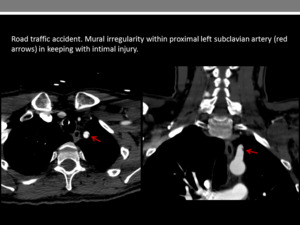
Fig. 2
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Complete wall defects
These include a defect through all three layers of the vessel wall (intima,
media and adventitia) resulting in active bleeding.
Alternatively a pseudoaneursym may form if there is a breach of the intima and media such that there is leakage of blood into a cavity that is contained by the adventitia,
with communication with the originating artery.
In some instances it can be contained by fibrous extravascular tissue formed as a response to trauma.
Typical CT appearances:
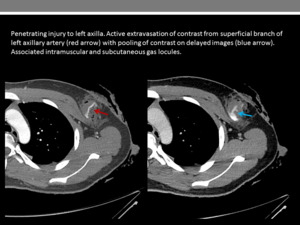
Fig. 3
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
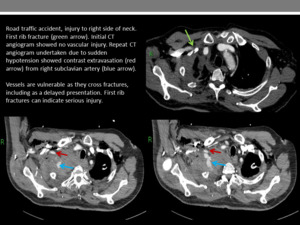
Fig. 4
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
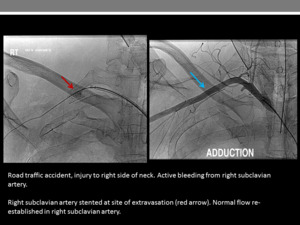
Fig. 5
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK

Fig. 6
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
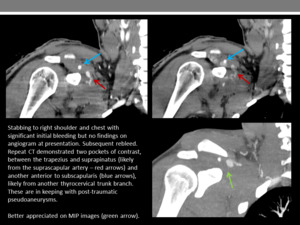
Fig. 7
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
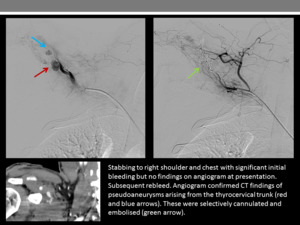
Fig. 8
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
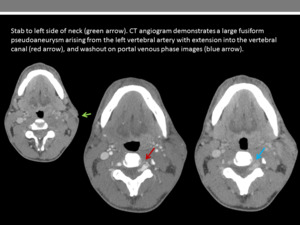
Fig. 9
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
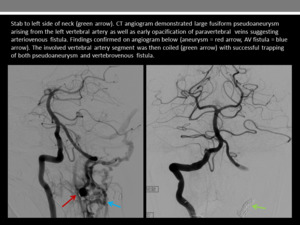
Fig. 15
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Transection
The vessel is torn completely or incompletely.
This can be associated with either (a) active haemorrhage,
in particular in cases of partial transection,
or (b) distal occlusion due to retraction and vasoconstriction.
It is more common in penetrating trauma.
Typical CT appearance:
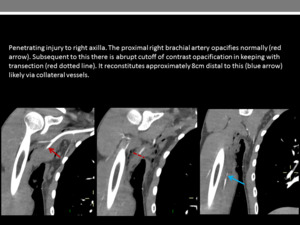
Fig. 10
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
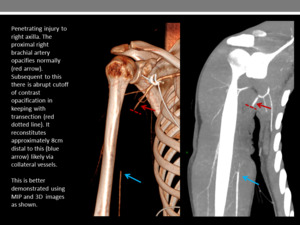
Fig. 11
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
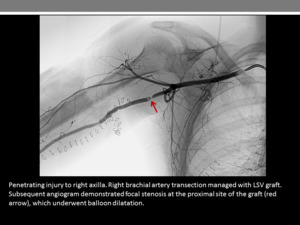
Fig. 12
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
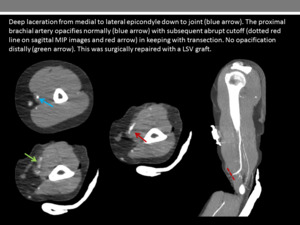
Fig. 13
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Arteriovenous fistula
Trauma can result in the development of an abnormal connection between the artery and an adjacent vein due to damage to these vessels,
bypassing normal anatomical capillary beds.
Typical CT appearance:
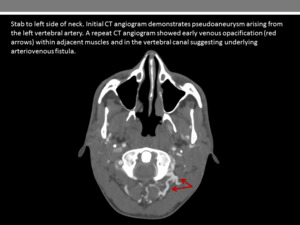
Fig. 14
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Fig. 15
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Contained haematoma
Pooling of blood adjacent to an injured vessel.
Typical CT appearance:
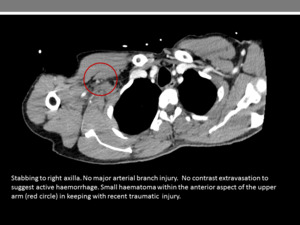
Fig. 16
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Vasospasm
Vasoconstriction can occur as a response to trauma,
causing decreased blood flow.
This may lead to functional damage distally.
It can occur more commonly in younger patients.
Typical CT appearance:
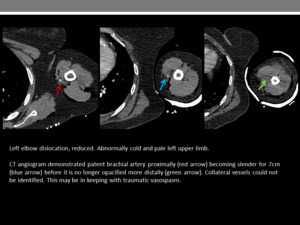
Fig. 17
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
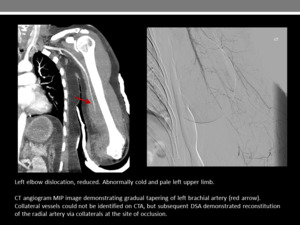
Fig. 18
References: Department of Radiology, Imperial College Healthcare NHS Trust, London / UK
Consequences of vascular injury [5]:
-
Blood loss
-
Ischaemia
-
Compartment syndrome
-
Tissue necrosis
-
Amputation
-
Death
