BILATERAL RENAL LESIONS : TUMORAL
1.
Nephroblastoma :
Male infant (6 y.o.) - Exploration of abdominal pain and parental palpation of an abdominal mass.
US shows bilateral renal masses,
slightly more echogenic than renal parenchyma.
MRI confirms bilateral renal tumors,
with the typical characteristics of nephroblastoma (hyperT2,
hypoT1,
heterogeneous enhancement).
Final diagnosis is bilateral nephroblastomas without metastasis,
probably part of a undefined syndrome (still currently being analyzed).
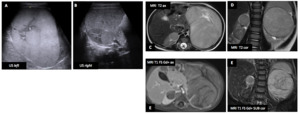
Fig. 1: Nephroblastoma : Male infant (6 y.o.)
Tips :
- Neuroblastoma (or Wilms tumor) is the most common pediatric renal mass,
typically occurring in early childhood (1-11 years) (80% before the age of 5 years) When part of a syndrome they occur often bilaterally even earlier,
typically between 2 and 24 months of age.
Cure up to 90% (thanks to surgery and chemotherapy).
- Typical imaging appearance : claw sign with the kidney ; US : heterogeneous masses (± cystic,
± calcifications (rare)) ; CT : heterogeneous soft-tissue masses with infrequent calcifications (~15%) and fat-density regions,
patchy enhancement,
lung metastases at time of diagnosis (20%) ; MRI : heterogeneous masses on all sequences (hypoT1,
hyperT2),
frequently containing blood products with heterogeneous enhancement.
- Examine (US,
MRI) the renal vein and inferior vena cava (IVC) and look for thrombosis (venous tumoral invasion is not rare) !
- DDx of pediatric abdominal masses closely related to kidneys include : neuroblastoma (calcifications are common,
encasing vascular structure without invasion,
poorly marginated,
lung metastases more common,
more commonly crosses the midline behind the aorta),
clear cell sarcoma (identical to very cystic Wilms tumor),
renal rhabdoid tumor (association with brain tumors,
especially in the posterior fossa).
2.
Acute lymphoblastic T leukemia :
Male patient (20 y.o.) - Exploration of asthenia,
dyspnea on exertion and purpura.
Blood labs revealed circulating T blast cells (89%) and chest X-ray a mediastinal mass (A).
CT showed mediastinal (D) and renal (B,
C) involvement (hypodense,
non enhancing nodular lesions).
These lesions disappeared (E) after chemotherapy and long term remission was obtained thanks to bone marrow allograft.
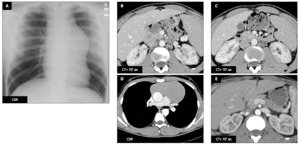
Fig. 2: Acute lymphoblastic T leukemia : Male patient (20 y.o.)
Tips :
- Leukemic infiltration (mostly Acute Lymphoblastic Leukemia (ALL)) up to 65 % at autopsy.
- Most common CT findings : diffuse bilateral infiltration with nephromegaly.
- CT and US findings are mostly common to infiltrative renal lymphoma ; unlike our case,
discrete renal masses are rare !
3.
Acute myeloid leukemia :
Male patient (21 y.o.) - Patient presented with cholestatic jaundice.
CT found a pancreatic head lesion (F-G-H-I-K : black ➙) with mass effect on CBD (I-J : red ➙) and dilatation of biliary tree and Wirsung duct.
Multiple diffuse hypodense renal bilateral lesions (A,
B,
L : blue ---) were uncovered.
All these lesions showed hypoT1 signal (C,
F) and restricted diffusion on MRI (D,
E,
G,
H).
A right humeral head lesion was also detected with PET-CT.
Renal biopsy revealed CD35+ CD45+ cells and medullary biopsy showed infiltration with 80% of myeloid blast cells.
Final diagnosis is AML (acute myeloid lymphoma).
Long term remission was obtained with aggressive chemotherapy.
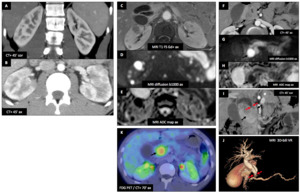
Fig. 3: Acute myeloid leukemia : Male patient (21 y.o.)
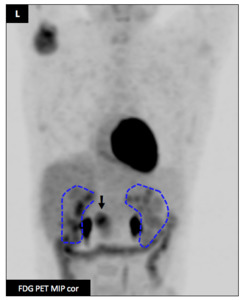
Fig. 4: Acute myeloid leukemia : Male patient (21 y.o.)
4.
Infiltrative lymphoma :
Male patient (52 y.o.) - Deterioration of general status revealing a mantle cell lymphoma with a large splenomegaly (E) (with splenic infarcts (A-E : red ➙)) (E) and lymph nodes,
kidneys,
pancreas and lung involvement (patchy ground glass opacities) (F).
All of these lesions were hypermetabolic (B,
C).
Swollen kidneys with cortical hypodense,
non enhancing patchy and diffuse nodular infiltration (A,
D) with hypermetabolism (B,
C).
No complete response obtained despite 3 aggressive lines of chemotherapy (GA101-DHAOx,
MATRix,
R-COPADEM).
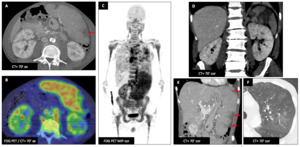
Fig. 5: Infiltrative lymphoma : Male patient (52 y.o.)
5.
Perirenal lymphoma :
Male patient (48 y.o.) - Incidental finding of a hyperlymphocytosis revealing a mantel lymphoma.
Morphological (A,
D) and metabolical (B,
C) imagings demonstrates multiple lymphadenopathies,
splenic and perirenal lymphomatous involvement (hypermetabolic,
hypodense rindlike soft tissue mass).
Complete response (E) obtained after immunochemotherapy (R-DHAOX),
stem cell autograft and under maintenance treatment (rituximab).
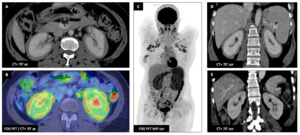
Fig. 6: Perirenal lymphoma : Male patient (48 y.o.)
Tips :
- Several renal lymphoma presentations exist : solitary or multiple masses,
perirenal involvement,
contiguous retroperitoneal extension,
diffuse infiltrative.
- Involvement is usually silent (i.e.
renal functions often unaffected).
Typical CT appearance : homogeneous,
hypodense,
minimal enhancing lesions.
- Vascular structures remain patent when the disease spreads and extends around them.
- Mass effect on excretory system may occur (especially with contiguous retroperitoneal extension of lymphoma).
6. Chromophobe renal cell carcinoma (ChRCC) :
Male patient (45 y.o.) - Incidental finding of bilateral renal mostly solid lesion (30 mm on the right and 67 mm on the left),
with well-defined central scar and necrosis.
Both lesions contain calcifications.
Enhancement is slightly heterogeneous and less important than normal adjacent renal cortex.
Total left nephrectomy and right tumorectomy was performed.
Pathological diagnosis was pure ChRCC on the right and mixed with oncocytoma component (hybrid tumor) on the left.
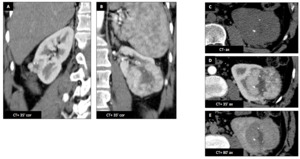
Fig. 7: Chromophobe renal cell carcinoma (ChRCC) : Male patient (45 y.o.)
Tips :
- Oncocytoma and ChRCC are radiologically indistinguishable.
Biopsy is often unhelpful as ChRCC may have oncocytic component.
Diagnosis is made on pathology after surgical resection.
- Invasive lesion (perirenal fat,
renal vein,
lymphadenopathy) favors ChRCC over oncocytoma.
- Typical CT oncocytoma / ChRCC appearance : enhancement more homogeneous than other RCC ; smaller enhancement than renal cortex and than ClRCC ; central scar /necrosis ; calcifications may be present.
7. Renal oncocytosis :
Male patient (80 y.o.) - Incidental finding of multiple bilateral renal tumors (cortical heterogeneous mass,
with maximal enhancement at nephrogenic phase (F)).
There was no invasion.
Surgical resection confirmed multiple oncocytomas of the biggest lesions and the others were stable 2 years after on control (not shown).
There was no skin papule and no lung cyst.
Germ line mutation of the Birt-Hogg-Dubé (BHD) syndrome gene was examined,
which failed to show any gene alteration.
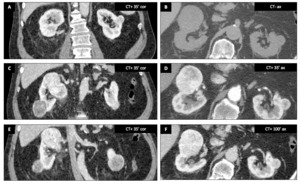
Fig. 8: Renal oncocytosis : Male patient (80 y.o.)
Tips :
- Neither CT nor MRI can differentiate oncocytoma from ChRCC !
- Multiple oncocytomas can be part of BHD syndrome or be an unrelated syndrome (oncocytosis / oncocytomatosis).
- Look for lung cysts that could be signs of lymphangioleiomyomatosis (LAM),
frequently present in BHD patients.
8.
Hereditary papillary renal cell carcinoma (PRCC) :
Male patient (48 y.o.) - Patient admitted to the ED with abdominal pain and distension.
Multiphasic CT scan demonstrates multiple bilateral renal masses,
mostly homogenous.
There was active bleeding (C-D-E : red ➙) complicating a large mass extending from the left kidney to the midline anteriorly.
Emergency left nephrectomy was performed.
Pathology revealed Hereditary Papillary Renal Cell Carcinoma (HPRCC).
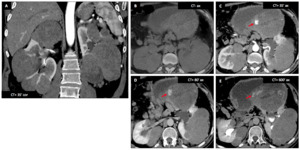
Fig. 9: Hereditary papillary renal cell carcinoma (PRCC) : Male patient (48 y.o.)
Tips :
- HPRCC is a rare AD genetic condition (mutation of MET gene) leading to multifocal papillary renal cell carcinoma (PRCC).
- It is difficult to differentiate PRCC from other RCC subtypes based on radiological studies.
- Other typical multi-focal RCC syndromes include von Hippel-Lindau (VHL) (ClRCC : typically higher enhancement and more heterogeneous than PRCC),
Birt-Hogg-Dubé (BHD) (ChRCC : no evident discriminative feature from PRCC).
Look for VHL and BHD other signs !
9.
Metastatic clear renal cell carcinoma (ClRCC) :
Female patient (86 y.o.) - The patient has a history of left ClRCC treated by partial nephrectomy (B : surgical clips).
Follow-up CT shows hypervascular left kidney masses (B) with large areas of necrosis,
without calcification,
with invasion of the renal vein (B : yellow ➙),
corresponding to clear cell renal carcinoma with metastases (right kidney (A : green ➙),
hepatic (F : orange ➙),
pancreatic (G : red ➙),
lymphadenopathies (C-D : blue ➙),
and lung nodules (E : purple ➙).
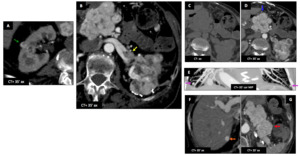
Fig. 10: Metastatic clear renal cell carcinoma (ClRCC) : Female patient (86 y.o.)
Tips :
| |
Degree of enhancement (most valuable parameter) |
Heterogeneity |
Calcifications |
Venous and perinephric invasion |
| ClRCC |
+++ |
++ |
+/- |
+ |
| ChRCC |
+ |
+/- |
+ |
- |
| PRCC |
+ |
+ |
+ |
+ |
| Collecting duct RCC |
+ |
+++ |
- |
++ |
9.
Transitional cell carcinoma :
Female patient (88 y.o.) - Patient admitted for deterioration of general condition and several episodes of fall.
Initial CT shows bilateral mucosal thickening of both renal pelvis (A-B-C : red ➙ ,
B : right renal pelvis,
C : left renal pelvis).
There is diffuse nodular infiltration of the peritoneal and retroperitoneal spaces corresponding to peritoneal carcinomatosis.
Because of cognitive disorders,
a palliative approach is chosen.
Final diagnosis is synchronous bilateral transitional cell carcinoma of the renal pelvis.
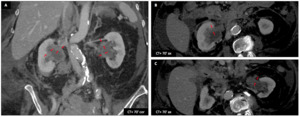
Fig. 11: Transitional cell carcinoma : Female patient (88 y.o.)
Tips :
- Transitional cell carcinoma (TCC) of the renal pelvis are 2-3x more common than the TCC of the ureter but 50x less common than bladder TCC,
probably because of the exposure of carcinogens in urine and urine stasis.
Synchronous lesions are rare.
Symptoms are non specific.
- Urine cytology is insensitive (positive in less than 20%).
- Typical CT appearance : soft tissue density lesions with mild enhancement centered on the renal pelvis (small focal mural thickening).
Kidney shape is often normal (in contrary to RCC).
Calcifications may be present.
Rarely TCC can be infiltrative (large hydronephrotic nonfunctioning kidney).
- Small lesions are difficult to detect : use late excretory phase enhancement and furosemide injection to obtain a better distension of the collecting system and to improve sensibility.
10.
Lung carcinoma metastases :
Male patient (56 y.o.) - Lung adenocarcinoma treated by lobectomy (A : left diaphragm elevation) relapses with lung (A : yellow ➙),
hepatic (B) and renal (A,
B) hypodense lesions corresponding to metastases.
Axillary lymphadenopathy is also visible (A : blue ➙ ).
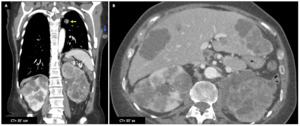
Fig. 12: Lung carcinoma metastases : Male patient (56 y.o.)
Tips :
- Kidney is a rare site of metastases (12th site in frequency).
Common primary neoplasms involved are : lung,
colorectal,
ENT,
breast,
soft tissue.
- Typical CT appearance : small,
multiple,
wedge-shaped,
less exophytic than RCC,
located within the renal capsule.
- When you discover multiple bilateral renal tumors,
search for a primary tumor !
11. Bourneville tuberous sclerosis (TS) :
Female patient (29 y.o.) - Bourneville Tuberous Sclerosis (TS) with multiple bilateral fat-containing lesions corresponding to multiple angiomyolipomas (AML).
Several arterial aneurysms required embolizations with coil to avoid bleeding complications.
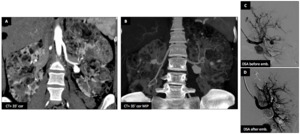
Fig. 13: Bourneville tuberous sclerosis (TS) : Female patient (29 y.o.)
Associated findings : pulmonary manifestations
- Lymphangioleiomyomatosis (LAM) : multiple thin-walled cysts scattered diffusely and surrounded by normal lung parenchyma.
- Presentation : in the 40s with dyspnea,
cough,
or hemoptysis.
- Complications : pneumothorax,
chylous effusion and ultimately respiratory failure.
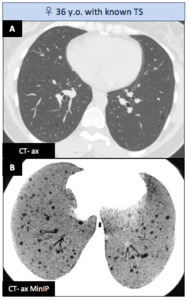
Fig. 14: Bourneville tuberous sclerosis - Associated findings : pulmonary manifestations
Associated findings : central nervous system (CNS) manifestations
- Subependymal Nodules : hamartomatous lesions lining the ventricles (hyperT1,
iso-hyperT2/FLAIR),
frequently calcified in the adulthood (C-E : red ➙).
- Cerebral White Matter Radial Migration Lines : heterotopic glial and neuronal cells along the path of migration from the ventricle to the cortex (hyperT2,
iso-hypoT1) (D : blue ➙).
- Cortical and Subcortical Tubers : disorganized neurons and glial cells and most commonly localized in the frontal lobes.
Their number is predictive of cognitive impairment (adults : hypoT1,
hyperT2/FLAIR ; infants : the opposite) (D-E : green ➙).
- Subependymal Giant Cell Astrocytomas : slow-growing,
enhancing lesions usually located at the foramen of Monro,
presenting in late childhood and arising from sub-ependymal nodules (F-G : 2013 ; H-I : 2016).
Distinction by MR spectroscopy is promising (not shown here).
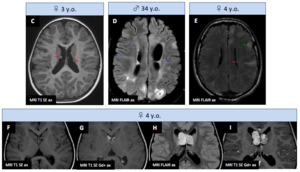
Fig. 15: Bourneville tuberous sclerosis - Associated findings : CNS manifestations
Tips :
- Renal manifestations of TS include AML (in 80% of TS patients ; 20% of patient with AML have TS),
renal cysts,
and renal cell carcinomas (RCCs) (incidence is similar to the general population but RCCs occur at much younger age and tend to grow more slowly).
- AML is the most common benign mesenchymal neoplasm composed of varying amounts of fat,
smooth muscle,
and blood vessels.
A small subtype of AML are lipid poor.
Arterial aneurysms are prone to develop with large AML.
- Typical lipid-rich AML semiology : US : homogeneously hyperechoic with posterior acoustic shadowing ; CT : with macroscopic fat and density less than -20 HU (pathognomonic) ; MRI : presence of fat confirmed on T1 FS and chemical-shift (india ink etching artifact at the fat-water interface between a lipid-rich angiomyolipoma and normal renal parenchyma).
- Lipid-poor AML : cannot be reliably differentiated from RCC and other renal tumors.
They are usually biopsied or closely followed.
- Increased risk of rupture/hemorrhage of AML > 4 cm or aneurysms > 5 mm = indication for embolization.
12.
Renal cysts :
Male patient (78 y.o.) - CT shows typical advanced Adult Dominant Polykystosis (ADPK) findings : multiple renal simple cyst,
renal parenchyma atrophy and liver cyst (A,
B,
C).
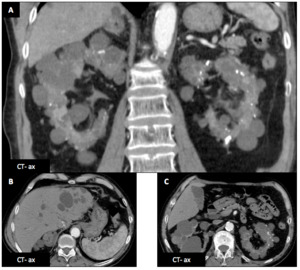
Fig. 16: Renal cysts : Male patient (78 y.o.)
Complications of renal cyst include (not on the same patients) :
- infection (D,
E) (infiltration around,
signs of pyelonephritis,
thickening of cyst wall),
- Hemorrhage (F,
G) (spontaneously dense,
non enhancing cyst),
- Malignant transformation (H-I : 2013 ; J : 2015) (apparition of wall tissular enhancing nodule = Bosniak 4 cyst ; ClRCC in this example).
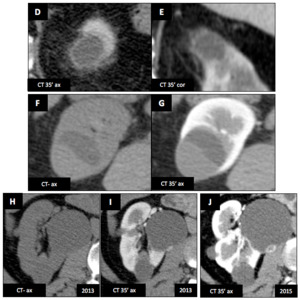
Fig. 17: Complications of renal cyst include (not on the same patient)
Another female patient (66 y.o.) - Another patient with ADPK (K,
L) : the cysts are smaller than the other patient (A,
B,
C) and renal parenchyma is less atrophic.
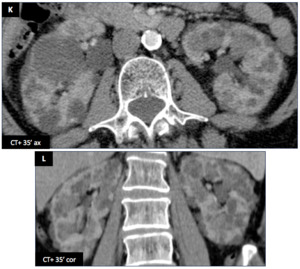
Fig. 18: Renal cysts : Another female patient (66 y.o.)
Tips :
- For renal cyst characterization and follow-up planning : use the Bosniak classification.
- Multiple bilateral renal cyst associated with hepatic cyst : think ADKP and seek brain aneurysm.
- Multiple bilateral renal cyst associated with pancreatic cyst : think VHL and seek ClRCC and CNS hemangioblastoma.
BILATERAL RENAL LESIONS : TOXIC/METABOLIC
12.
Acute cortical necrosis :
Male patient (38 y.o.) - Contrast-enhanced CT demonstrates a non-enhancing renal cortex (A-B : red ➙) with persistent medullary enhancement (cortico-medullary inversion) in a patient with a history of recent methanol ingestion.
Very subtle cortex corticis is visible (B : yellow ➙).
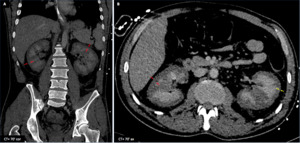
Fig. 19: Acute cortical necrosis : Male patient (38 y.o.)
Tips :
- Typical CT appearance : normal kidneys on native CT but cortico-medullary inversion on contrast enhanced CT.
- Cortical rim sign (cortex corticis) may be seen (very subtle in this case).
- Other etiologies include : severe hemodynamic shock,
microangiopathic hemolysis,
renal transplantation,
snake bites.
Female patient (35 y.o.) - Renal failure after hemodynamic shock (retroplacental hematoma) : natural course of cortical necrosis.
- CT day+8 : Hypodense cortex.
- CT day+16 : Swollen,
non enhancing hypodense cortex.
Cortical rim sign (cortex corticis).
Medulla is normally enhanced after contrast injection.
- MRI day+35 : Low signal intensity on both T1 and T2 weighted sequences affecting the inner renal cortex and the columns of Bertin with cortical liquefactive necrosis.
Cortical rim sign persists.
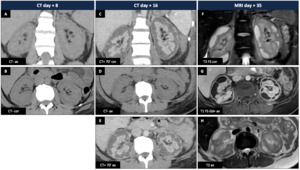
Fig. 20: Acute cortical necrosis : Female patient (35 y.o.)
Teaching point : the "Cortex corticis" or "Cortical rim sign"
- Most of renal parenchyma receives its arterial blood through main renal artery/arteries.
- Most peripheral part of the cortex is also vascularized by capsular arteries coming from diaphragmatic,
lumbar,
renal,
gonadal arteries and/or directly from the aorta.
- In case of abnormal perfusion of the main renal artery or of some of its branches,
there may be infarction of renal parenchyma relying on these arteries but salvage of the peripheral part of the cortex (cortex corticis) thanks to the capsular perforating branches.
This cortical rim sign (red ➙) is not always clearly visible.
- Cortical rim sign or cortex corticis is a specific (but non sensitive) finding for differentiating infarction from nephritis.

Fig. 21: Teaching point : the "Cortex corticis" or "Cortical rim sign"
References: Nicolas Villard
13.
Paroxysmal nocturnal hemoglobinuria :
Male patient (65 y.o.) - Mild renal insufficiency in a patient known for paroxysmal nocturnal hemoglobinuria (PNH).
CT shows normal kidneys (A,B).
On MRI,
renal cortex is hypo-T2 (C) and shows hyposignal on in-phase sequence (shorter TE,
1.5 T) (D) with higher cortical T1 signal on out-phase (longer TE,
1.5T).

Fig. 22: Paroxysmal nocturnal hemoglobinuria : Male patient (65 y.o.)
Tips :
- MRI must be performed facing renal failure with normal CT and US appearance in patient with hemolytic disease !
- Diagnosis of iron overload is possible by using “dual-sequence” (gradient in- and out-of-phase) : decreased signal intensity in the affected tissues on the in-phase (longer TE) images compared with the out-of-phase (shorter TE) images (this is only true for 1.5 T MRI scans).
- Always look for thrombosis in patient with PNH as it is a common and fatal complication !
14. Oxalosis :
Male patient (24 y.o.) - Patient known for untreated primary type 1 hyperoxaluria (confirmed by liver biopsy) is hospitalized for terminal renal failure.
Abdominal plain radiograph,
renal ultrasonography (hyperechoic medullary) and CT reveals large confluent medullary calcifications.
Renal cortex is atrophic,
dense and showed some very subtle calcifications.
The patient underwent sequential liver-kidney transplant.
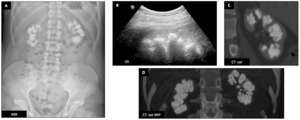
Fig. 23: Oxalosis : Male patient (24 y.o.)
Tips :
- Hyperoxaluria is characterized by nephrocalcinosis and nephrolithiasis because of supersaturation of calcium oxalate in urine.
- Primary hyperoxalurias (PH) are genetic disease and as the defective enzyme is liver specific in PH1,
sequential liver-kidney transplant is the definitive treatment.
- Imaging shows renal atrophy with extensive nephrocalcinosis (usually involving cortex and medulla).
- Extra-renal oxalate crystals deposits may be seen in moycardium,
bowel wall.
Bone abnormalities may be seen.
15.
Cacchi-Ricci disease :
Female patient (31 y.o.) - Patient known for several urinary lithiasis episodes with no electrolytes abnormalities.
Ultrasound control revealed pyramidal diffuse hyperechogenicity (C) compatible with nephrocalcinosis.
Abdominal plain field demonstrates no significant renal calcifications.
CT shows dense pyramids (white pyramid sign) (B).
Intravenous pyelography (IVP) (A) shows paintbrush appearance of distal tubules (D = zoom of A : red ➙) and confirms the diagnosis of Cacchi-Ricci disease.
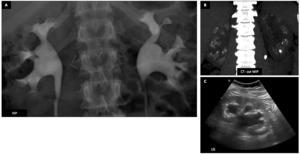
Fig. 24: Cacchi-Ricci disease : Female patient (31 y.o.)
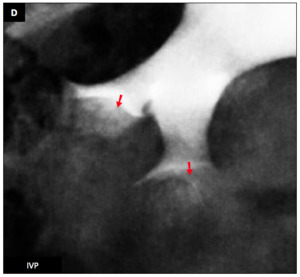
Fig. 25: Cacchi-Ricci disease : Female patient (31 y.o.)
Tips :
- Cacchi-Ricci disease or Medullary sponge disease (MSD) is a developmental anomaly that often remains asymptomatic.
Patient are prone to urinary lithiasis.
- US demonstrates echogenic medullary pyramid (whether or not nephrocalcinosis is present).
- Non contrast CT may show the white pyramid sign.
- IVP shows typical cystic dilatation of distal collecting tubules containing calcifications called bunch of grapes or bouquet of flowers with characteristic streaky appearance of dilated distal tubules called paintbrush appearance.
Teaching point : semiology of Cacchi-Ricci :
Another patient with distal collecting tubules containing calcifications (bunch of grapes or bouquet of flowers) (E : green ➙) with streaky appearance of dilated distal tubules called paintbrush appearance after contrast injection (F,
G : red ➙).
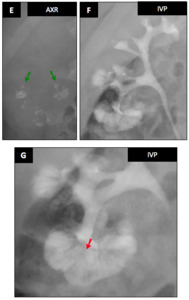
Fig. 26: Teaching point : semiology of Cacchi-Ricci disease
16. Lithium kidneys :
Male patient (70 y.o.) - Patient known for a bipolar mood disorder present with signs and symptoms of progressive chronic renal failure and diabetes insipidus.
MRI revealed innumerable uniformly distributed kidney microcyst.
Some common simple larger cyst are visible too (without relation with lithium).
Renal biopsy demonstrates tubular atrophy chronic interstitial nephritis,
glomerulosclerosis and distal tubular dilatation with microcyst compatible with a lithium induced nephropathy.

Fig. 27: Lithium kidneys : Male patient (70 y.o.)
Tips :
- Oral lithium is a very common treatment for depressive or mood disorder with a narrow therapeutic window.
Adverse effects include hypothyroidism,
teratogenicity,
dehydration and kidney damage.
- Consider lithium toxicity when a patient presents with renal failure and multiple uniformly distributed renal microcysts.
- Ultrasound shows normal sized kidneys with increased echogenicity.
On CT (often unenhanced because of the chronic renal failure),
the microcyst are difficult to detect.
- Lithium nephropathy is best highlighted using MRI,
especially bili-MRI T2 sequences with MIP ! Gadolinium is not useful.
17.
Extramedullary hematopoiesis :
Male patient (72 y.o.) - Staging workup for a pancreatic adenocarcinoma revealed nodular perirenal fat infiltration.
Nodular components show no enhancement but MR signal drop in opposition phase sequences.
Iron deposition in erythroid tissue is responsible for blooming artifact on MR TRUFI sequence.
Biopsy demonstrated no tumoral cells and confirmed blood immature precursor cells.
Final diagnosis was perirenal extramedullary hematopoeisis in chronic anemia background.
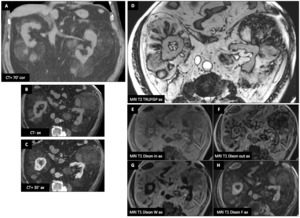
Fig. 28: Extramedullary hematopoiesis : Male patient (72 y.o.)
Tips :
- Extramedullary hematopoeisis (EMH) is the production of blood element in abnormal locations (thorax,
abdomen,
CNS) due to various causes of chronic anemia (bone marrow replacement,
myelofibrosis,
hemoglobinopathies,
etc.).
- Perirenal space is a site of hematopoeisis during fetal life.
- Imaging appearance : CT : hypodense heterogeneous hypovascular mass on CT.
US : distinct solid mass with internal vascularity.
MRI : heterogeneous mass with variable T1 and T2 signal ; fat component is typical (interest of chemical shift imaging) ; GE is useful for detecting hemoglobin derived products.
BILATERAL RENAL LESIONS : VASCULAR
18. Bilateral venous thrombosis :
Male patient (54 y.o.) - CT performed in the context of a systemic septic shock (no urinary source) shows bilateral hypo-perfused swollen kidneys with a poor cortico-medullary differentiation.
There is IVC thrombus (A : red ➙) extending bilaterally in both renal veins (A-C : red ➙).
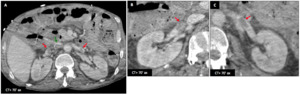
Fig. 29: Bilateral venous thrombosis : Male patient (54 y.o.)
Comparative case : unliateral left renal vein thrombosis
Left renal vein thrombosis (D : red ➙).
is detected in a 19 y.o.
♀ with a inferior vena cave (IVC) malformation (partially shown here).
Left kidney is mildly swollen and relatively hypodense because of the venous stasis.
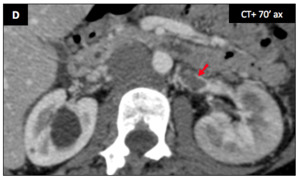
Fig. 30: Comparative case : unliateral left renal vein thrombosis
Tips :
- Always check venous permeability,
especially in the context of systemic shock.
- Bilaterally hypo-perfused kidneys may be difficult to detect (because of the symmetry).
- US findings : renal enlargement with hypoechoic cortex from edema (early phase) ; atrophy and increased echogenicity (late).
- Doppler findings : reversal of arterial diastolic flow,
high resistive index in the renal artery,
absent venous flow.
- CT findings : enlarged kidney,
changes in attenuation (focal or diffuse) due to perfusion abnormalities,
persistent cortical enhancement and lack of parenchymal enhancement,
collateral vessels (late).
19.
Fibromuscular dysplasia :
Male patient (58 y.o.) - Follow-up of renal artery fibromuscular dysplasia.
CT shows bilateral cortical notches (sequels) on both kidneys (A : green ➙).
Dysplastic renal arteries with vascular loops,
fusiform vascular ectasia and alternance of stenoses and dilatations,
best seen on maximum intensity projections (MIP) (B-C : red ➙).
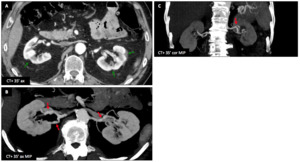
Fig. 31: Fibromuscular dysplasia : Male patient (58 y.o.)
Another female patient (59 y.o.) - Another 59 y.o.
female patient with extended arterial renal dysplasia (with well visible string of beads appearance on the right renal artery (D : blue ➙)),
but without parenchymal lesion.
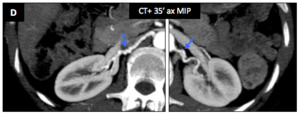
Fig. 32: Fibromuscular dysplasia : Another female patient (59 y.o.)
Tips :
- Fibromuscular dysplasia (FMD) affects small and medium caliber arteries (more often the renal,
carotid and vertebral arteries).
- Important role of radiologist for early recognition and shortening of the delay between symptoms and final diagnosis.
- Imaging findings : string of beads appearance,
vascular loops,
fusiform vascular ectasia,
arterial dissection,
aneurysm and subarachnoid hemorrhage.
20. Renal infarcts - Buerger disease :
Male patient (43 y.o.) - The patient is a male smoker known for a distal thromboangiitis of lower limbs.
In 2013,
MRI arteriography (A) showed distal arterial stenosis and occlusion (A : green ➙) with typical corkscrew collaterals (A : red ➙).
In 2017,
he presented with acute kidney injury (AKI),
bilateral lombalgia and acute hypertension.
CT (B,
C) and MRI scans (D) revealed bilateral renal lesions corresponding to multiple infarcts.
There was no argument for an immune cause on biochemical tests.
Final diagnosis is thromboangiitis obliterans (Buerger disease) with renal infarctions.
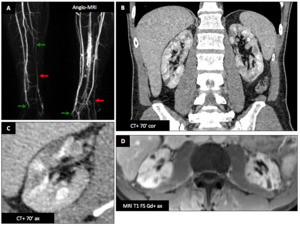
Fig. 33: Renal infarcts - Buerger disease : Male patient (43 y.o.)
Tips :
- Thromboangiitis obliterans is an occlusive,
inflammatory,
non-necrotizing,
non-atherosclerotic vasculitis causing ischemia of small and medium vessels.
- Strong association with smoking !
- Typical angiographic features : extensive arterial occlusion,
corkscrew collateral vessels,
both limbs involved,
sparing of larger inflow vessels.
- Diagnosis needs exclusion of diabetes,
autoimmune causes and embolization.
21. Polyarteritis nodosa :
Male patient (35 y.o.) - Acute left flank pain associated with decreased hemoglobinemia.
Emergency CT shows a left perirenal posterior hematoma (A).
CT after contrast injection reveals several rounded hyperdense addition images on renal arteries corresponding to aneurysms (B-C-D : red ➙).
On of them seems to be related to the hematoma (D : green ➙) (focal rupture).
No active bleeding was noted.
There are small bilateral cortical infarcts.
Angiography (E,
F) confirmed bilateral beading and numerous microaneurysms affecting the segmental and interlobar arteries.
Final diagnosis is polyarteritis nodosa (PAN),
confirmed by pANCA measurement.
Full remission was achieved corticosteroids and cyclophosphamide
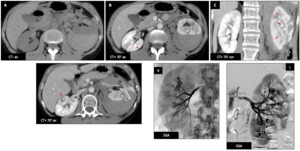
Fig. 34: Polyarteritis nodosa : Male patient (35 y.o.)
Tips :
- Polyarteritis nodosa (PAN) is a systemic inflammatory necrotizing vasculitis that involves small to medium sized arteries (larger than arterioles).
- More common in male around the 5th to 7th decades.
- Association with Hepatitis B in 20-30 % of the cases.
- The association of arterial microaneurysms with cortical infarcts is suggestive of PAN.
Another male patient (47 y.o.) - Patient presenting an inflammatory syndrome with abdominal diffuse pain,
proteinuria and hypertension.
ANCA measurement is positive.
CT and angiography demonstrates multiple characteristic microaneurysms in both kidneys (B-C-D-E : red ➙).
There is no significant anomaly of the rest of the visceral arteries (F).
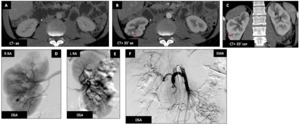
Fig. 35: Polyarteritis nodosa : Another male patient (47 y.o.)
Tips :
- Renal arteries are the first vessels to be involved.
- Renal damage and complications are a major cause of death.
- Pulmonary circulation is typically spared,
although bronchial arteries may occasionally be involved.
BILATERAL RENAL LESIONS : INFECTIOUS
22.
Pyelonephritis - Renal abcesses nodosa :
Female patient (63 y.o.) - Right kidney is swollen,
hypodense and partially dedifferentiated.
Left kidney has normal size but shows subtle cortical triangular and linear hypodense lesions (A-B-C : green ➙) (uncomplicated pyelonephritis).
There is a simple cortical cyst at the superior pole of right kidney (B-C-D : white *).
Images E and D show apparition of foci of abscess 7 days later (d + 7 days) (E-D : red ➙) (complicated pyelonephritis).
Favorable evolution occurs after appropriated antibiotherapy (F to H) : constitution/organization of the abscesses (F : d + 13 days),
progressive resolution of these collections (G : d + 28 days) and sequels (parenchymal thinning and renal cortical scars seen as notches) (H : d + 4 months).
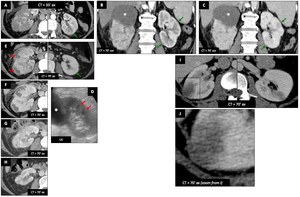
Fig. 36: Pyelonephritis - Renal abcesses : Female patient (63 y.o.) (A-H) and another female patient (59 y.o.) (I-J)
Another female patient (59 y.o.) - Patient with bilateral uncomplicated acute focal bacterial nephritis.
Unlike cortical infarction,
cortex corticis (cortical rim sign) is absent (J is a zoom from I rectangle).
Tips :
- Urinary tract infection is a clinical diagnosis and imaging is only indicated for : male patients,
pregnant women,
diabetic or immunocompromised patient,
history of stones or prior renal surgery or not responding to therapy after 7hours.
- Uncomplicated infection of renal parenchyma presentations on CT : hypodense cortical triangle (typical pyelonephritis),
striated cortical hypodensities (striated nephritis),
focal hypodense rounded cortical lesion without liquefaction (acute focal bacterial nephritis).
- Uncomplicated infection of pyelitis : thickening and enhancement of pyelic mucosa.
- Acute complications : abscesses and obstruction.
23. Renal tuberculosis :
Male patient (52 y.o.) - Extrapulmonary tuberculosis with Pott disease,
peritoneal,
renal and vesical bladder involvements.
Because of bladder perforation and secondary infections,
double-loops were placed.
- Left kidney : pseudotumoral TB with some mass-like ; irregular calix erosions (moth-eaten calix (A-E : red ➙)) and uneven caliectasis (some are not opacified on the late acquisition due to exclusion by stricture).
- Right kidney : end-stage TB with renal atrophy and dystrophic calcifications.
- Bladder : atrophy with diverticula and parietal thin calcifications (C).
- Spine : signs of spondylodiscitis with end plate mirror erosions and reactive sclerosis (beginning of resolution) (B).
Microbiological cultures confirmed M.
tuberculosis infection.
Clinical improvement occurs after anti-tuberculosis quadritherapy introduction.
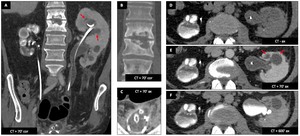
Fig. 37: Renal tuberculosis : Male patient (52 y.o.)
References: Dr. G. Lecoanet (CHRU Nancy, France)
Tips :
- Renal tuberculosis accounts for 15-20% of extra-pulmonary tuberculosis.
- Two subsets of renal parenchyma involvement exists : pseudotumoral form (mimicking RCC) and pyelonephritis.
- The collecting system is the most common site of urinary tuberculosis with multifocal stricture causing uneven caliectasis leading eventually to hydronephrosis.
The involved bladder becomes distorted,
thickened and shrunken.
- Inadequately treated,
atrophy of the renal parenchyma and hydronephrosis progress,
the kidney appears as multiple thin-walled cysts or as a multiloculated cyst.
The end-stage is dystrophic calcifications involving both entire kidneys,
known as “putty kidney”.
24. Candidiasis :
Female patient (61 y.o.) - Patient with acute lymphoid leukemia (AML) treated by chemotherapy with medullar aplasia presents a persistent fever despite antibiotic therapy.
CT shows multiple random lung nodules (B) and multiple hepatic,
splenic and renal small hypodense nodules (A,
C,
D) in favor of microabscesses.
Analysis confirmed systemic candidiasis.
All these findings disappeared after Fluconazole treatment.
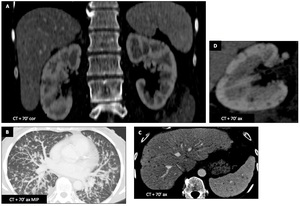
Fig. 38: Candidiasis : Female patient (61 y.o.)
Tips :
- Invasive Systemic candidiasis is the most common invasive fungal infection in hospitals,
with high mortality.
- In immunocompromised patients with fever despite large antibiotherapy,
look for fungal infection : CT and MRI have a great sensibility to detect signs of candidiasis.
- Typical CT visceral involvement findings are multiple small round low-attenuation lesions distributed randomly.
- Pulmonary candidiasis CT presentation depends of the routes for spread,
which in our case is most compatible with hematogenous spread (multiple miliary nodules).
BILATERAL RENAL LESIONS : SYSTEMIC
25. Birt-Hogg-Dubé syndrome :
Male patient (53 y.o.) - Patient with skin papular lesions on the face is followed-up for recurrent bilateral chromophobe RCC and oncocytomas with several lesions surgically resected and a history of pneumothorax.
Molecular biology studies confirmed Birt-Hogg-Dubé (BHD) syndrome.
CT shows bilateral cortical renal masses (A,
B,
C).
Left kidney was reimplanted into left iliac fossa during one of the precedent tumor removal.
The masses are natively isodense to renal parenchyma (A).
After contrast injection (B,
C,
H,
I),
the enhancement is homogeneous and less important than normal renal cortex.
Thoracic CT shows signs of lymphangioleiomyomatosis (LAM) (multiple lung cyst of different sizes with normal parenchyma in between) (D,
E).
On MRI,
the lesions are iso-T1 (F),
contain no fat (F,
G) and restrict diffusion (J,
K).

Fig. 39: Birt-Hogg-Dubé syndrome : Male patient (53 y.o.)
Tips :
- It is important to include BHD syndrome in the DDx for every patient with bilateral renal tumors and lung cysts.
- Look for typical cutaneous manifestations of BHD (papules on face).
- Oncocytoma (benign) and ChRCC (malignant) are radiologically indistinguishable.
BHD patients are prone to oncocytomas,
ChRCC and hybrid tumors.
- LAM is a risk factor for pneumothorax and chylous effusion.
BHD imaging recommendations : due to high risk of renal cancers,
yearly US or CT/MRI every 2 years is recommended (beginning at age of 25 years).
26.
von Hippel-Lindau (VHL) syndrome :
Female patient (24 y.o.) - Multiple renal masses,
some containing cystic component / Bosniak 4 cysts (e.g.
: blue ➙ and red ➙) corresponding to ClRCC in a VHL patient.
There are multiple simple renal (Bosniak 1) (e.g.
orange ➙) and pancreatic cysts without pejorative criteria (e.g.
green ➙).
This combination of two kind of renal cysts (benign and malignant) is typical of VHL.
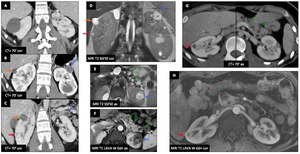
Fig. 40: von Hippel-Lindau (VHL) syndrome : Female patient (24 y.o.)
Tips :
- VHL patients are likely to develop multiple pancreatic (serous cysts and serous cystadenomas of pancreas) and kidney benign cysts (Bosniak 1).
But they are also at risk for RCC and neuroendocrine pancreatic tumors.
Pancreas cysts are almost specific for VHL.
- Look carefully for atypical renal cyst : cyst’s wall nodule,
pseudocapsule on T2,
enhancement on T1 Gd+,
solid lesion.
Close and careful follow-up is mandatory : annual renal screening (US±CT/MRI) is recommended.
- Preferred treatment for VHL disease-associated RCC is nephron-sparing procedures (partial nephrectomy,
percutaneous ablation).
- Other VHL tumors include : retinal/CNS hemangioblastoma,
pheochromocytoma,
pancreatic NET,
papillary cystadenoma of the epididymis and endolymphatic sac tumor,
…
Associated findings : CNS : Hemangioblastoma
Female patient (63 y.o.) with known VHL disease : headaches,
vertigo and vomiting revealing right cerebellar mass on MRI.
Lesion is mainly cystic,
with a small mural nodule with cystic spaces itself,
(E) hypervascular (A,
B) with important neoangiogenesis (high CBV (C)) and T2 serpentine flow void.
Feeding arteries are visible on nodule periphery after Gd injection.
There is a large mass effect on the 4th ventricle.
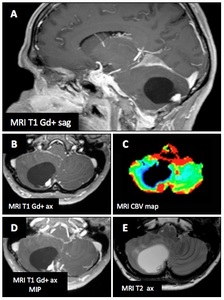
Fig. 41: vHL - Associated findings : CNS : Hemangioblastoma
Tips :
- Typical sites are cerebellum,
spinal cord and medulla.
- Recommendations : baseline MR imaging at the age of 20.
Associated findings : Adrenal glands : Pheochromocytoma
Young female patient (10 y.o.) with known VHL disease : 10 y.o.
♀ with known VHL disease : hypertensive crisis revealing secondary hypertension.
Urinary catecholamines were positive.
123I-MIBG SPECT (A,
C) showed high uptake at the right adrenal gland.
There is a right adrenal mass,
heterogenic,
hyperT2 (light bulb sign (B)),
hypo-T1,
without fat component (no signal drop in out-phase sequence) (D,
E).
There is pathognomonic enhancement (> +120 HU) after iodinated contrast injection (F,
G).
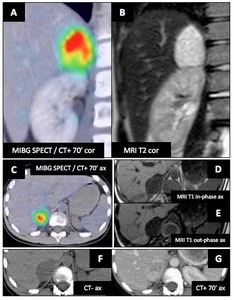
Fig. 42: vHL - Associated findings : Adrenal glands : Pheochromocytoma
Tips :
- Recommendations : Laboratory screening annually (24h measurement of urine vanillylmandelic acid level).
- MRI (hyperT2,
hypoT1,
strong enhancement) is superior to CT.
- MIBG SPECT is highly sensible and specific and help to locate metastases.
Associated findings : Pancreas : Neuroendocrine tumors
Female patient (39 y.o.) with known VHL disease : Follow-up revealed a small (10 mm) growing pancreatic hypervascular,
hypoT1,
hyperT2 lesion,
with restriction of diffusion in the head of pancreas.(A-D : red ➙) Patient was asymptomatic.
This is the typical appearance of neuroendocrine tumor (NET).
Image E show multiple cystic lesion of pancreas tail.
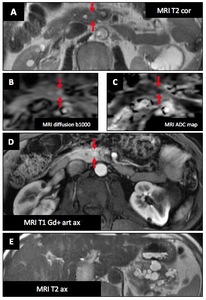
Fig. 43: vHL - Associated findings : Pancreas : Neuroendocrine tumors (Female patient (39 y.o.))
Another male patient (34 y.o.) with known VHL disease : Another example of pancreatic NET.
CT shows two hypervascular lesions (A-E : red ➙ and green ➙),
not visible on unenhanced CT (A).
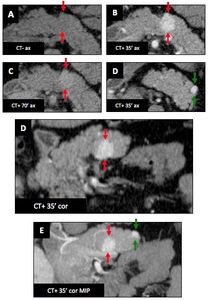
Fig. 44: vHL - Associated findings : Pancreas : Neuroendocrine tumors (Male patient (34 y.o.))
Tips :
- Recommendations : No specific screening guidelines exist.
- NET more frequent in VHL patients with pheochromocytoma.
- Good prognosis ! Frequency of metastases and malignancy of NET in VHL is low (<10%),
whereas sporadic NET metastasize in more than 60% of cases.
- Typical imaging appearance : CT- : iso/hypodense ; CT+ : intense arterial enhancement ; MRI : relative hyperT2.
27.
Erdheim-Chester disease :
Male patient (48 y.o.) - Discover of hairy kidneys (A,
B,
C) on CT during work-up for arthralgia.
On FDG PET,
there is a significant FDG uptake in the proximal and distal part of both tibias and in the proximal part of the humerus (D : red ➙).
There is diffuse articular uptake too.
On bone scintigraphy HDP-99mTc,
there are intense early and late uptakes in the proximal and distal parts of tibias and in the proximal part of the humerus (E-F : red ➙).
Lower limb MRI show bilateral medullary T1 and proton density (PD) hypersignals with enhancement after Gd injection.
HyperPD signal of the anteromedial periosteal region of the tibia is suggestive of periosteitis (I : green ➙).
Bone biopsy (tibia) confirmed Erdheim Chester disease.
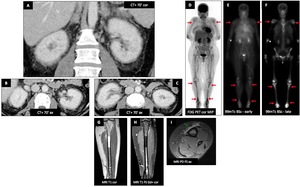
Fig. 45: Erdheim-Chester disease : Male patient (48 y.o.)
Brain MRI reveals swelling of extra-ocular muscle,
exophthalmos (A) and retro-ocular pseudotumoral infiltration (B : red ➙) with intraconal masses enhancing after Gd injection (C : green ➙).
Cardiac MRI demonstrates infiltration of the right atrio-ventricular groove (D-E : orange ➙) and of the inter-atrial septum (D-E : blue ➙).
Final diagnosis is Erdheim Chester disease (ECD) with bone,
orbital,
perirenal and cardiac involvement.
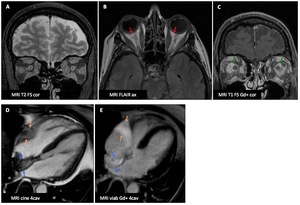
Fig. 46: Erdheim-Chester disease : Male patient (48 y.o.)
Another male patient (41 y.o.) - Contrast-enhanced CT images of the abdomen shows bilateral perirenal soft tissue infiltration (hairy kidney appearance) (A-B : red ➙).
Presence of soft tissue infiltration (C : green ➙) covering the aorta (coated aorta appearance).
MRI (D) : homogeneous enhancement of soft tissue lesions (white asterisk) in the retrobulbar space which entraps the optic nerves bilaterally.
Bone scintigraphy (E) :
1.
Static tissue image : hyperhaemia of both tibia.
2.
Static bone image : heterogeneous bone fixation of both tibia.
Immunohistochemistry (F) : CD68+,
a typical marker of ECD.
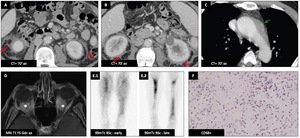
Fig. 47: Erdheim-Chester disease : Another male patient (41 y.o.)
References: Dr Nicolas Alberti, CLCC Bergonié, Bordeaux, France
Tips :
- ECD is a rare non-Langherans cell non familial multisystemic granulomatosis.
Common presenting symptom is bone pain.
- MSK involvement : bilateral and symmetric metaphyseal and diaphyseal sclerosis of the long bones (mostly the tibias ; increased uptake on Tc-MDP bone scan.
Most common involvement.
- Visceral involvement : lung (can mimic Langherans cell histiocytosis),
hairy kidneys,
retro-orbital masses,
cardiac and aorta infiltration.
- CNS involvement : meninges infiltration,
hypothalamus or pituitary masses,
peri-arterial infiltration.
- Mortality reaches 60% despite aggressive treatment (lung and cardiac failure).
Radiologist has a key role to shorten the delay to the final diagnosis.
28. Retroperitoneal fibrosis :
Male patient (83 y.o.) - CT of a patient known for stable Waldenström macroglobulinemia.
There is diffuse retroperitoneal periaortic fibrous infiltration extending in the perirenal spaces,
corresponding to retroperitoneal fibrosis (RPF) (A,
B,
C,
E).
FDG PET (D) demonstrates small metabolic activity.
The ureters are trapped into this fibrosis and show irregular caliber on the excretory acquisition (F)).
On follow-up imaging 3 years later (not shown),
the RPF mildly progressed.
Because no biopsy was performed,
differential diagnosis remains open between secondary and primary RPF.
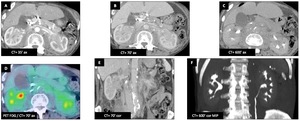
Fig. 48: Retroperitoneal fibrosis : Male patient (83 y.o.)
Tips :
- RPF is a rare disease hallmarked by inflammation and deposition of fibrous tissue around the aorta.
It can be primary (Ormond’s disease) or secondary (malignancies,
drugs,
IgG4 disease,
infections,
injuries,
radiotherapy,
surgery).
- Imaging studies fail to differentiate primary from secondary RPF.
FDG PET has a role for identifying active and quiescent fibrotic infiltration.
- DDx of perirenal infiltrations include lymphoma,
RPF,
Erdheim Chester disease.

