ECR 2018 / C-2917
Fishing the pulmonary nodule: CT-guided hook wire localization
Congress:
ECR 2018
Poster Number:
C-2917
Type:
Educational Exhibit
Keywords:
Interventional non-vascular, Thorax, Lung, CT, Percutaneous, Diagnostic procedure, Surgery, Multidisciplinary cancer care
Authors:
M. R. Calero Garcia1, G. GARCIA GALARRAGA1, N. Pérez Peláez2, M. De la Puente Herraiz1, A. B. Enguita Valls1, J. C. Meneses Pardo1; 1Madrid/ES, 2Madrid, Madrid/ES
DOI:
10.1594/ecr2018/C-2917

Fig. 1

Fig. 2

Fig. 3

Fig. 4
")
Fig. 5:
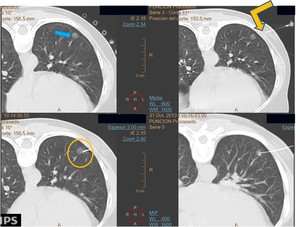
The puncture point is determined using the CT gantry lights and the grid on the...
. Scan is performed as deemed necessary to check the needle progression. Tip of the introducer cannula in the chest wall,before entering the pleural cavity, correctly alineated with the lesion (yellow arrow), and then reaching the lesion edge (yellow circle), The final scan despite the correct position of the hook-wire into the nodule.")
Fig. 6:
Initial Ct scan shows a 10mm ground-glass nodule in the left lowerlobe (blue...

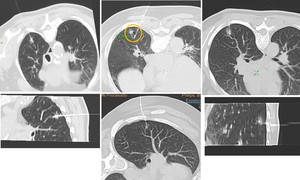
Fig. 7:
Differents patterns of correct hook wire emplacement

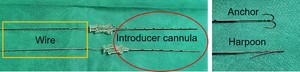
Fig. 8:
We use wires with an extreme anchor shaped or harpoon shaped.

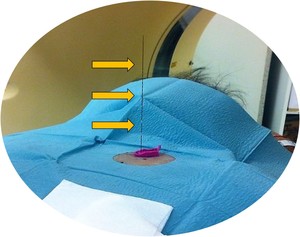
Fig. 9:
Wire extending outside the chest wall.
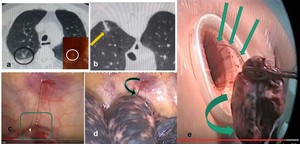
 Nodule location. b) Hook wire placement. c),d),e) VATS procedure and tumor extraction with hook wire inside.")
Fig. 10:
a) Nodule location. b) Hook wire placement. c),d),e) VATS procedure and tumor...

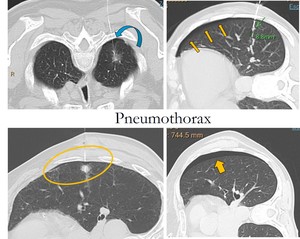
Fig. 11:
Pneumothoraces are adjacent to the pleural puncture site and laminar puncture...
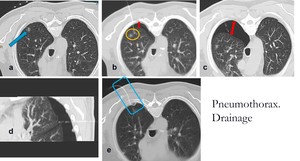
 nodule location. b) hook wire placement (nearby the nodule) and small pneumothorax. c/d) growing pneumothorax with hook wire dislodgement to pleural cavity. e) pigtail (placement in CT room) and pneumothorax impprovement.")
Fig. 12:
a) nodule location. b) hook wire placement (nearby the nodule) and small...

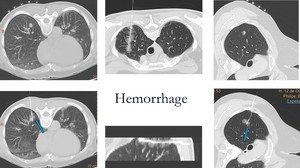
Fig. 13:
Mild hemorrhage along the hook-wire traject or around the lesion