Idiopathic intracranial hypertension (also known as pseudotumor cerebri and benign intracranial hypertension) is a disorder of increased cerebrospinal fluid (CSF) pressure of unknown cause.
Previously it was commonly known as pseudotumor cerebri because of common clinical signs of intracranial hypertension without tumoral causes.
The overall incidence of idiopathic intracranial hypertension is approximately between 2 and 19 per 100,000.
It mostly occurs in young women in childbearing age who are obese (with a body mass index above 25).
Pathogenesis and etiology of idiopathic intracranial hypertension
The pathophysiology of this condition is poorly understood.
Several pathophysiological mechanisms regulating cerebrospinal fluid (CSF) pressure have been postulated.
Some of the proposed mechanisms are: inflammatory factors in correlation to obesity,
increased cerebral blood volume,
excessive CSF production,
venous outflow obstruction and compromised CSF resorption.
Obesity and female gender are the strongest and most consistent risk factors of IIH.
Moreover,
some studies suggest that weight gain,
as opposed to initial BMI,
is the leading factor of poor visual outcome.
This finding accentuates cross-links between weight gain and high cerebral venous pressure in the pathogenesis of IIH.
One of the possible pathophysiological mechanisms for raising intracranial pressure in obese patients could be the increased intraabdominal pressure resulting in reduced cerebral venous drainage.
Furthermore,
chronic inflammation associated with obesity can lead to a prothrombotic state which contributes to development of IIH.
On the other hand,
adipose tissue is an actively secreting endocrine tissue.
One of the long-standing hypotheses for the pathogenesis of IIH cites abnormal vitamin A metabolism as well as elevated levels of retinol found in CSF in some patients with IIH.
Therefore,
there is a possible correlation between adipose tissue,
vitamin A production and development of IIH.
Other possible agents in pathogenesis of IIH are sex hormones because of preferential occurrence of the disorder among postpubertal,
pre-menopausal women,
and the absence of a gender preference before puberty.
The transverse sinus stenosis (TSS) theory is widely spread and much discussed,
but it is still unclear whether it could be a cause or a consequence of IIH.
This theory supports obstruction of the intracranial venous drainage as a main pathophysiological mechanism for IIH.
ICP can be raised due to secondary causes such as:
- Cerebral venous abnormalities - dural venous sinus thrombosis,
bilateral jugular vein thrombosis,
superior vena cava syndrome,
arteriovenous fistula
- Decreased CSF absorption from a previous intracranial infection or subarachnoid hemorrhage
- Exposure to or withdrawal from certain exogenous substances - tetracycline,
antibiotics,
amiodarone,
levodopa,
ketoprofen,
lead,
lithium,
vitamin A, retinoids,
anabolic steroids,
withdrawal from chronic corticosteroids
- Endocrine disorders (Addison disease,
hypoparathyroidism),
metabolic disorders,
systemic disease
Clinical presentation
IIH is characterized by increased intracranial pressure (ICP) leading to headache,
papilledema,
visual symptoms and signs without any lateralizing findings in the neurological examination,
and normal CSF findings.
The most prominent clinical finding in patients with IIH is papilledema which may be bilateral,
asymmetrical,
or even unilateral.
However,
in some cases IIH can occur in the absence of papilledema.
These patients,
without papilledema may experience a headache profile similar to chronic daily headache with migrainous features,
responding well to specific antimigraine agents.
The patients with papilledema can develop serious visual impairment and eventually blindness.
The condition must be taken seriously and adequate treatment must follow the diagnosis.
Typical IIH clinical presentation and findings are:
- Headache
- Transient visual obscurations
- Photopsia,
diplopia,
visual disturbance (acuity and/or field loss) and blindness
- Sudden visual loss
- Symptoms of increased intracranial pressure
- Retro-orbital pain
- Pulsatile tinnitus
- Radicular pain
Headache is one of the leading symptoms.
It is usually progressive with at least one of the following characteristics: daily occurrence,
diffuse and/or constant (non-pulsating) and aggravated by coughing or straining.
In some cases the headache may be accompanied with allodynia,
typically in unilateral V1 distribution.
Since the headache can mimic migraine the diagnosis of IIH can be difficult.
Transient visual obscurations occur in most patients as a symptom of papilledema.
The disturbance can last up to 30 seconds and is described as a dimming or blackout of vision in one or both of the eyes.
They are often predominantly orthostatic.
Diplopia is typically horizontal caused by sixth nerve palsy.
Sudden visual loss may happen due to intraocular hemorrhage secondary to peripapillary subretinal neovascularization related to chronic papilledema.
Radicular pain is an uncommon symptom,
typically localized in the arms.
Friedman et al.,
proposed recently updated Dandy criteria for the diagnosis of IIH which are presented in Table.1.
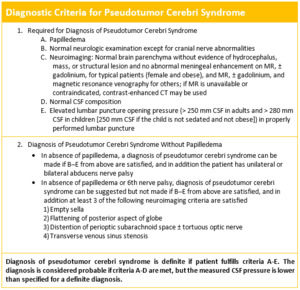
Table 1
References: University Hospital, Sisters of Charity University Hospital - Zagreb/HR
Treatment
The optimal management usually creates problems for clinicians.
It ranges from simple dietary measures to neurosurgical and endovascular procedures.
Not all patients require treatment.
In general,
severe headache and evidence of optic nerve involvement are reasons to initiate the treatment.
Since the disease can lead to severe visual impairment and eventually blindness the main therapeutic goal is to preserve optic nerve function.
First line treatment is weight loss in obese patients.
The dietary measurements are usually accompanied with pharmacologic therapy – acetazolamide and furosemide for lowering ICP; amitriptyline,
propranolol for primary headache prophylaxis; and,
in some cases corticosteroids for lowering ICP.
The therapeutic role of repeated lumbar punctures which were popular in the past is now questioned due to its difficulties for the patient and lack of evidence showing any long lasting effects.
Surgical interventions include optic nerve sheath fenestration and CSF diversion procedures including either lumboperitoneal or ventriculoperitoneal shunting.
In patients with bilateral TSS unilateral TSS stenting appears to be a safe and effective treatment.
