Arachnoid Cyst
Arachnoid cysts are benign,
congenital,
intraarachnoidal space-occupying lesions that are filled with clear CSF and tend to be unilocular,
smoothly marginated expansile lesions without communication with the ventricular system.
Most arachnoid cysts are supratentorial.
- The best diagnostic clue is a sharply demarcated extraaxial cyst that can displace or deform adjacent brain.
Scalloping of the adjacent calvarium is often seen.
- The classic arachnoid cyst has no internal architecture,
does not enhance and typically has the same signal intensity as CSF at all sequences.
The most difficult lesion to distinguish from the arachnoid cyst is an epidermoid cyst.
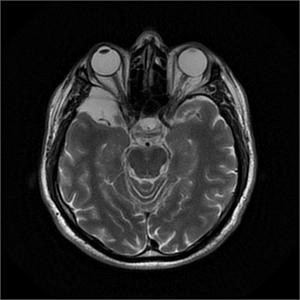
Fig. 1: T2WI shows arachnoid cyts in right middle cranial fossa causes scalloping of posterior orbital bony wall.
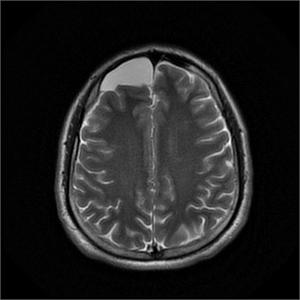
Fig. 2: Arachnoid Cyst is seen in right anterior cranial fossa on T2WI.
Abscess
Brain abscess is localized infection of brain parenchyma due to typically bacterial infection.
Fungal or parasitic infections are less common causes of brain abscess.
Typically location is supratentorial brain.
Frontal lobe involvement due to sinusitis,
and odontogenic infection or temporal lobe involvement due to otomastoiditis is common.
In case of hematogenous dissemination (pulmonary infection,
endocarditis etc),
grey-white matter junction involvement is seen.
Multipl lesion may be seen due to septic emboli.
- MR is the best imaging modality.
Well-defined,
thin-walled enhancing rim with diffusion restriction is common imaging findings.
T2 hypointense rim is surrounded by edema.
Cystic primary tumors or metastases should be considered in differential diagnosis list.
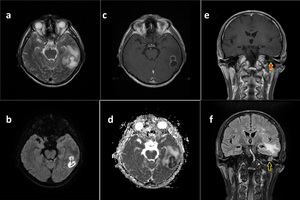
Fig. 3: Abscess.
Axial T2WI shows left cystic lesion with hypointense rim and perilesional edema in adjacent white matter (a).
DWI and ADC map shows prominent restriction(b, d).
Axial T1WI after gadolinium reveals enhancing rim (c). Findings are consistent with abscess.
Coronal T1WI after gadolinium (e) and coronal FLAIR sequences (f) show inflamatory changes in left timpanic cavity, the most likely cause of abscesss.
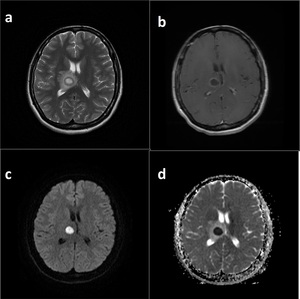
Fig. 4: Abscess. T2WI shows right thalamic cystic lesion with distinct perilesional edema (a).
DWI and ADC maps show prominent restriction in internal component of the lesion (c, d)
T1WI after gadolinium demostrates hypointense rim of the lesion. Findings are consistent with abscess (b).
Cavum Septi Pellucidi (et Vergae)
Cavum septi pellucidi (CSP) is cystic cerebrospinal fluid (CSF) cavity cavity of septum pellucidum and occurs with or without cavum vergae (CV).
CSP is usually depicted as elongated finger shaped CSF collection between lateral ventricles,
usually measured under 1 cm diameter.
CV is defined as posterior extension of CSP between fornices.
- CSF imaging findings in cavitary area is seen on all modalities.
Sagittally,
CSP extends from rostrum to splenium of corpus callosum.
Asymmetrical lateral ventricles,
cavum velum interpositum may be considered in differentials.
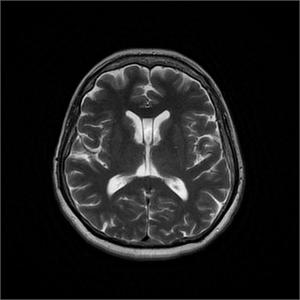
Fig. 5: Cavum Septum Pellucidi et Vergae.
Cavum Velum Interpositum
Cavum velum interpositum (CVI) is defined as triangular shaped midline CSF space over thalami.
Apex point of CVI points toward foramen of Monroe,
roof of CVI elevates fornixes and bottom of CVI flattens-displaces internal cerebral veins inferiorly.
- CVI imaging finding are same as the CSF on CT or MR sequences.
Slit-like triangular shape is typical.
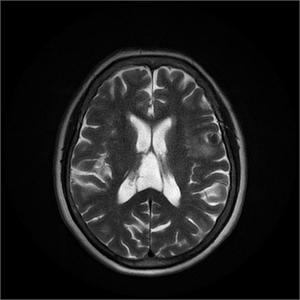
Fig. 6: Cavum Velum Interpositum. T2WI shows slit-like triangular shaped cerebrospinal fluid space.
Colloid Cyst
Colloid cysts are benign mucin-containing cysts and account for 15%–20% of intraventricu- lar masses.
They are mostly found in the foramen of Monro.
The cysts are typically attached to the anterosuperior portion of the third ventricular roof and may produce sudden acute hydrocephalus.
The cysts are smooth and round,
varying in size.
The mean size is 1.5 cm.
They consist of mucin,
blood degradation products,
foamy cells,
and cholesterol crystals.
- Colloid cyst appears as a well-delineated hyperattenuated mass on nonenhanced CT scans in foramen Monroe.
- On T1-weighted MR images,
two- thirds of colloid cysts are hyperintense.
The majority are isointense to brain on T2-weighted images.
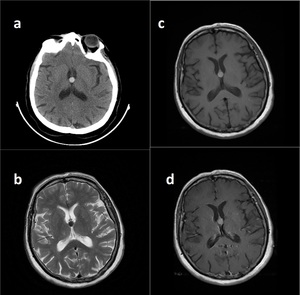
Fig. 7: Colloid Cyst. CT demostrates well delineated hyperdense mass in foramen Monroe (a).
T2WI reveals low T2 signal (b) whereas on T1WI, lesion is seen as hyperintense mass due to its mucinous compounds (c).
Post-gadolinium T1WI shows no enhancement.
Coroid Plexsus Cysts
Choroid plexus cysts (CPCs) are non- neoplastic epithelial-lined cysts of the choroid plexus.
They are the most common of all intracranial neuroepithelial cysts.
Mostly they are bilateral and located in the lateral ventricular atria.Their size is measuring 2–8 mm in diameter.
- CPCs are usually hyperintense to CSF on T2WI.
The majority do not become completely hypointense on FLAIR images and remain moderately hyperintense to CSF.
- Mostly they are iso or hyperintense on precontrast T1WI compared with CSF and show rim or nodular contrast enhancement.
The major differential diagnosis is ependymal cyst and villous hyperplasia of the choroid plexus.
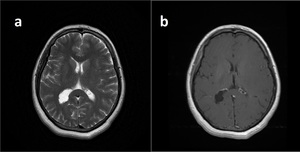
Fig. 8: Choroid Plexsus Cyst.
T2WI shows lobulated cystic lesion in the atriumof the rigt lateral ventricle (a).
Post-gadolinium T1WI demostrates thin, slightly enhancing cyst walls.
Craniopharyngioma
Chraniopharyngioma is a benign,
often partially cystic sellar region tumor derived from rathle pouch.
Chraniopharyngioma is divided in two types : Adamantinomatous (childhood cystic mass) and Papillary (solid mass in older adults).
- Chraniopharyngioma generally multilobulated,
often large (>5 cm). On CT cystic lesion with calsification and enhancing walls with contrast medium is typical.
- MR signal depends on cystic component.
T1 may be hyperintense due to high protein content,
therefore,
T1W and T2W signals are variable.
Rathke cleft cyst,
pituitary adenoma,
suprasellar arachnoid cyst ar in differentials.
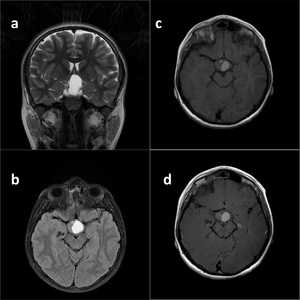
Fig. 9: Craniopharyngioma. Coronal T2WI reveals suprasellar lobulated masss indenting base of the 3th ventricle and optic chiasm (a).
On FLAIR image, lesion is seen hyperintense due to its proteinaceous compounds.
Pre- and post-gadolinium (c, d) T1W images show no internal enhacement, proving its cystic structure.
Cystic Metastasis
The most common sources of intracranial metastases in order of decreasing frequency are carcinomas of the lung,
breast,
malignant melanoma,
carcinomas of the kidney,
and carcinomas of the gastrointestinal tract.
Some of them have central necrosis,
and intratumoural haemorrhage is found in about 20% of cases.
- On MRI examination,
most intracerebral metastases show decreased signal onT1WI and increased signal on T2WI.
T1WI after administration of gadolinium is the most sensitive method for evaluation of intracranial metastases,
because the lesions are almost always enhanced,
appearing as ring,
punctuate,
or solid.
- On CT scan without enhancement,
the tumours are difficult to be detected due to their discrete appearance as rounded homogeneously isodense or hyperdense nodules,
surrounded by extensive vasogenic oedema,
seen as hypodensity of the cerebralmatter .
Rim-enhancing necrotic or cystic lesion image is sensitive but not specific.
Brain abscesses in their capsular stage can demonstrate similar findings.
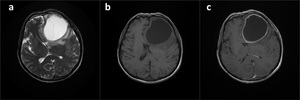
Fig. 10: Cystic Metastasis. T2WI, pre- and post-gadolinium T1W images demostrates left frontal cystic mass lesion with enhancig wall (a, b, c). Lesion proved to be the low differentiated carcinoma metastasis.
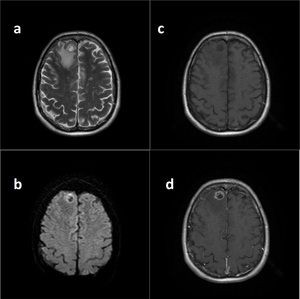
Fig. 11: Cystic Metastasis.
T2WI shows right frontal cystic lesion with perilesional edema (a).
DWI reveals partly restriction in the lesion (b).
Pre-and post-gadolinium T1W images demostrate prominent enhancig rim (c, d). Findings are consistent with metastasis in this patient with known history of primary lung cancer.
Dermoid Cyst
Dermoid cysts are congenital ectodermal inclusion cysts,
extremely rare,
and are less common than epidermoid cysts.
They tend to occur in the midline sellar,
parasellar,
or frontonasal regions .
Growth can lead to rupture of the cyst contents,
causing a chemical meningitis that may lead to vasospasm,
infarction,
and even death.
Characteristically,
the cyst contains secretion of sebaceous glands and desquamated epithelium.
The cysts may also contain hair and/or teeth.
- Dermoid cysts are hyperintense on T1WI and do not enhance.
The masses have heterogeneous signal intensity on T2WI.
Fat signal or density,
calcium contents are important diagnostic clues.
Dermoid cysts may be confused with an epidermoid,
craniopharyngioma,
teratoma,
or lipoma.
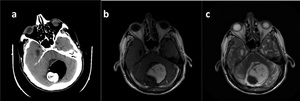
Fig. 12: Dermoid Cyst.
CT shows extra-axial, retro-cerebellar mass lesion with gross calsification and fatty components (a).
T1WI and T2WI show hypointense calsification and hyperintense fatty components compatible with CT findings (b, c).
Dandy-Walker Continuum
Dandy Walker Continuum is represent broad spectrum of posterior fossa malformations.
Thereare five types defined from the most severe to the least severe,
as follows:
- Classic Dandy-Walker Malformation (CDWM) is defined as cystic dilatation of 4th ventricle with enlarged posterior fossa.
Vermi is seen as hypoplastic and rotated superiorly.
- Hypoplastic vermis with rotation: Variable vermian hypoplasia is seen.
Posterior fossa and brainstem are sized normally.
Keyhole vallecular is typical.
- Persistan Blake pouch cyst: Open 4th ventricle communicates with cyst.
Primary fissure,
posterior fossa,
brainstem ar senn normal.
- Mega cisterna magna: Enlarged pericerebellar cisterns communicate with basal subarachnoid spaces.
Imaging findings are variable due to type of malformation.
Large posterior fossa with rotated vermis should alert radiologist.
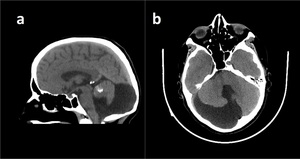
Fig. 13: Hypoplastic Vermis with Rotation.
CT shows normal-sized posterior fossa (a). Brainstem is also normal sized (not shown). Keyhole vallecula is seen on axial image (b).
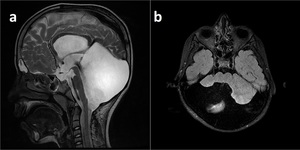
Fig. 14: Classic Dandy-Walker Malformation with enlarged posterior fossa (a), hypoplastic cerebellar hemispheres and absent vermis (b).
Encephalomalacia
Encephalomalacia is defined as regional brain parenchymal damage. Findings are often subtle; ventriculomegaly should alert radiologist as a first clue.
- Diffusely abnormal high T2 signal in brain parenchyma indicates edema an also foci of low T2 signal may represent hemorrhagic areas.
Schizencephaly and arachnoid cyst should be considered as differentials.
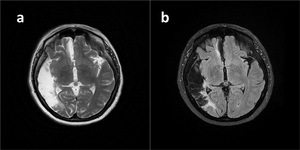
Fig. 16: Encephalomalacia.
A large right temporoparietal cystic cavity is seen on T2WI (a) and there is gliotic hyperintense signal on FLAIR (b) in adjacent brain parenchyma. Findings are consistent with sequale findings of right MCA infarction.
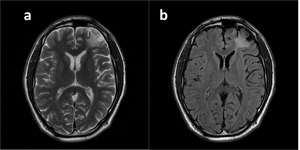
Fig. 15: Encephalomalacia.
T2W (a) and FLAIR (b) images show left frontal cortical cystic lesion with perilesional gliotic hyperintensity consistent with trauma sequale.
Enlarged Perivascular Space
Enlarged PVSs,
also known as Virchow- Robin spaces,
are pial-lined interstitial fluid-filled structures that accompany penetrating arteries and veins.
They are common,
incidental,
“leave me alone” lesions that should not considered as candidate for intervention.
They frequently appear in the inferior basal ganglia,
clustering around the anterior commissure and surrounding the lenticulostriate arteries.
Enlarged PVSs are considered a normal variant.
- They appear as smoothly demarcated fluid-filled cysts,
typically less than 5 mm in diameter,
and often occur in clusters in the basal ganglia or midbrain.
They are isointense to CSF at all sequences,
including FLAIR.
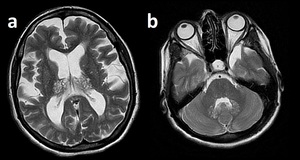
Fig. 17: Enlarged PVS.
Bilateral thalamic (a) and dentate (b) enlarged PVSs in a patient with Mucopolisacaridosis.
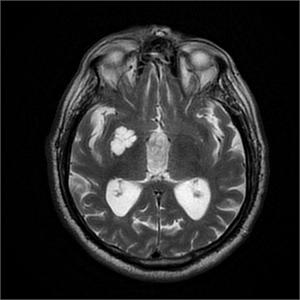
Fig. 18: Enlarged PVS.
T2WI demostrates enlarged PVS as a lobulated cystic structure in sublentiformic area .
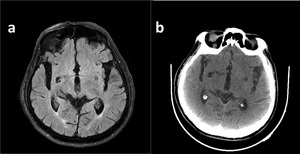
Fig. 19: Enlarged PVS around right anterior comissura shown on FLAIR (a) and axial CT image(b). Note CSF like appereance on both modalities.
Ependymal Cyst
Ependymal cysts are rare,
benign,
ependymal-lined cysts of the lateral ventricle or juxtaventricular region of the temporoparietal region and frontal lobe.
They are thin walled and filled with clear serous fluid secreted from ependymal cells.
- The best diagnostic clue is a non-enhancing thin-walled CSF-containing cyst of the lateral ventricle.
The differential diagnosis for an ependymal cyst includes choroid plexus cyst,
arachnoid cyst,
neurocysticercosis,
and asymmetric ventricles.
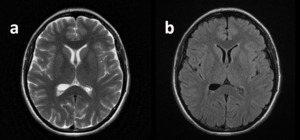
Fig. 20: Ependimal Cyst is located in atrium of right lateral ventricle on T2WI (a) and FLAIR image (b).
Epidemoid Cyst
Intracranial epidermoid cysts are congenital inclusion cysts and are four to nine times as common as dermoid cysts.
The most common location for epidermoid cysts is the cerebellopontine angle cistern.
They are the third most common overall cerebellopontine angle cistern.
- The best diagnostic clue is a CSF-like mass that insinuates within cisterns,
encasing adjacent nerves and vessels.
- Most epidermoid cysts are isointense or slightly hyperintense to CSF on T1WI and T2WI.
They do not suppress completely on FLAIR images and restrict on DWI.
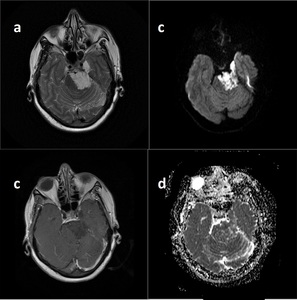
Fig. 21: Epidemoid Cyst. T2WI (a) shos cystic lesion at prepontin cistern and perimesencephalic area. Post-gadolinium images reveals no enhancing component(b). DWI (c) and ADC (d) demostrates difusion restriction.
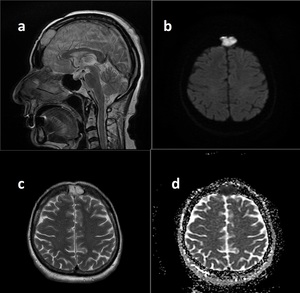
Fig. 22: Sagittal and axial T2WI (a, c) shows intradiploic hyperintense lesion.
DWI (b) and ADC map demostrate difusion restriction. Findings are consistent with intradiploic epidemoid cyst.
Hippocampal Remnant Cyst
Hippocampal remnant cysts represent partially unfused hippocampal sulcus.
It occur due to an embryologic defect in cornu ammonis and dentate gyrus fuse.
- These cysts are incidental and not associated with pathology.
Cyst may enlarge due to Alzheimer’s Disease.
- Typical cystic findings are demonstrated on MR and CT.
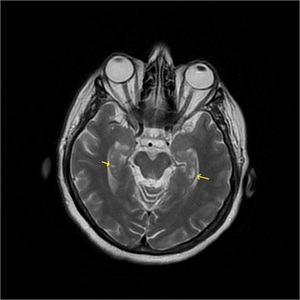
Fig. 23: Bilateral Hippocampal Remnant Cysts are seen on T2WI (yellow arrows).
Lacunar Infarct
Lacunar infarcts are small,
deep cerebral infarcts located in basal ganglia and thalamus,
pons or cerebral white matter.Common locations are deep gray nuclei,
particularly putamen,
thalamus and caudate nuclei.
The size of the lacunar infarct may be measured up to 15 millimetres.
Risk factors are cerebrovascular disease,
hypertension,
diabetes,
and hypercholesterolemia.
- Small,
well circumscribed areas of parenchymal abnormality in basal ganglia and white matter is common imaging finding.
- Cyst-like internal signal with gliotic rim on FLAIR is typical.
Prominent perivascular space encountered in differentials.
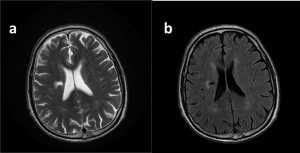
Fig. 24: Rigt periventricular cystic (a) lesion with gliotic border on FLAIR (b). Findings are consistent with lacunar infarct.
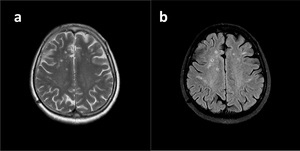
Fig. 25: Small periventricular cystic cavities with characteristic imaging findings of lacunar infarct on T2WI (a) and FLAIR image (b).
Leptomeningeal Cyst (Enlarging Calvarial Fracture)
Leptomeningeal cyst is actually a misnomer definition of enlarging calvarial fracture adjacent to post-traumatic encephalomalacia.
- A lineer lytic skull lesion with scalloped margins is characteristic definition.
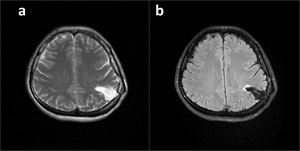
Fig. 34: T2WI (a) and FLAIR (b) show left parietal leptomeningeal cyst adjacent to the old fracture line and protruding to the calvarium.
Neuroglial Cyst
Neuroglial or glioependymal cysts are benign epithelial-lined lesions that occur anywhere in the neuraxis .
They are representing fewer than 1% of intracranial cysts.
Frontal lobe is the most typical location.
- The best diagnostic clue to a neuroglial cyst is a nonenhancing CSF-like parenchymal cyst with no surrounding abnormal signal intensity.
The cysts are benign appearing lesions with smooth,
rounded borders.
Other lesions that may be mistaken for a neuroglial cyst include an enlarged PVS,
infectious cyst,
porencephalic cyst,
and arachnoid cyst.
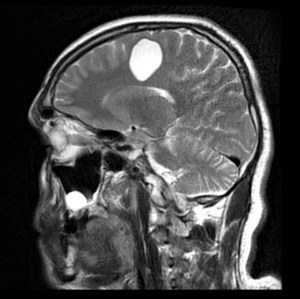
Fig. 26: Neuroglial Cyst located in right frontal lobe.
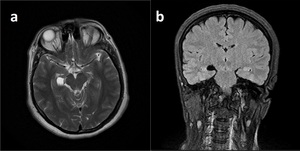
Fig. 27: Neuroglial Cyst located at right chroid fissure is shown on axial T2WI and coronal FLAIR (b)
Porencephalic Cyst
Porencephalic cysts are congenital or acquired cavities within the cerebralhemisphere that usually communicate directly with the ventricular system.
They can be cortical or subcortical,
unilateral or bilateral.
Congenital porencephalic cysts originate from a fetal or perinatal process that results from intrauterine vascular or infectious injury.
Acquired cysts are secondary to injury later in life and are usually secondary to trauma,
surgery,
ischemia,
or infection.
- They are typically CSF-filled cavities with a smooth wall and are lined with gliotic or spongiform white matter.
- The typical porencephalic cyst communicates brain parenchyma with an enlarged adjacent ventricle.
The cysts have the same appearance as CSF at all MR sequences.
The differential diagnosis for the porencephalic cyst includes arachnoid cyst,
schizencephaly,
ependymal cyst,
encephalomalacia,
and hydranencephaly.
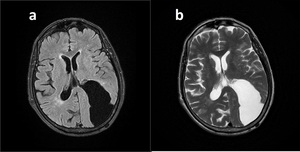
Fig. 28: Porencephalic Cyst.
There is a cleft-like cystic cavity in left parietoocipital lobes connecting lateral ventircle to the subarachnoid space. Gliotic signal is seen on FLAIR (a) alongside the parenchymal borders. Note the absence of grey matter lining on T2WI (b).
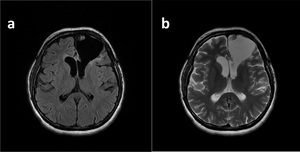
Fig. 29: Porencephalic Cyst. Cleft-like cystic cavity in left frontal lobe demostrates typical findings of porencephalic cyst on FLAIR (a) an T2W (b) images.
Pineal Cyst
Pineal cysts and cystic degeneration of the pineal gland with some residual pi- neal parenchyma are common; they are seen in up to 10% of cases at routine imaging.
Eighty percent are smaller than 1 cm in diameter.
Cysts larger than 1.5 cm may result in hydrocephalus.
- The best diagnostic clue is unilocular fluid- filled mass within the pineal gland.
- Attenuation or signal intensity depends on cyst content.
Rim or nodular calcium in the cyst wall on may be seen.
- Nodular enhancement is also common.
On T1-weighted MR images,
55%–60% are slightly hyperintense to CSF.
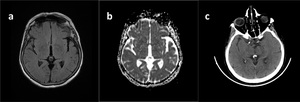
Fig. 30: Pineal Cyst.
FLAIR (a) and ADC (b) demostrates cystic lesion with CSF-like signal charasteristics. Axial CT image (c) reveals mural calsification.
Rathke’s Cleft Cyst
Rathke cleft cysts are congenital non-neoplastic cysts arising from remnants of the embryonic Rathke cleft.
They are common incidental intrasellar and suprasellar lesions.
Rathke cleft cysts arise from the failure of obliteration of the Rathke pouch.
- They are smoothly marginated cysts that vary in size from a few millimeters to 1–2 cm.
The contents vary from clear CSF-like fluid to dense mucoid material.
- The best imaging clue is a nonenhancing noncalcified sellar region cyst with an intracystic nodule.No enhancement is senn after contrast material administration.
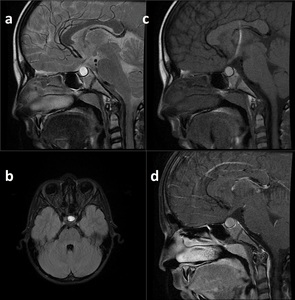
Fig. 31: Rathke Cleft Cyst.
Hyperintense on T2W (a), FLAIR (b) and pre-contrast T1W image due to internal contents. Post-contrast T1WI (d) demostrates no enhancement.
Schizencephaly
Schizencephaly is a cleft in brain parenchyma that extend from cortical surface to ventricle or in other words,
from pia to ependyma.
It is lined by dysplastic gray matter.
It is thought to be a result of acquired in utero neuronal migration.
- Transmantle gray matter lining cleft in all modalities are typical.
- It is usually located in frontal and parietal lobes near the central sulcus.
MR is the best choice of imaging.
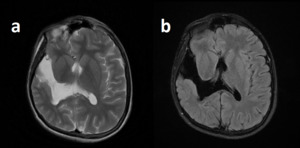
Fig. 32: Schizencephaly.
T2WI (a) and FLAIR (b) demostrates right temporal cystic cavity connecting right lateral ventricle to subarachnoid space. Note the displastic gray matter lining.
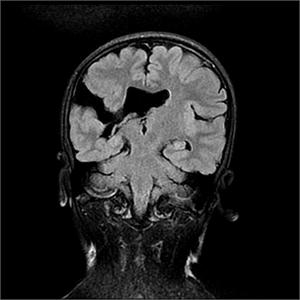
Fig. 33
