# DIRECT SIGNS OF THROMBOSIS
-The positive findings of intraluminal thrombus are the most important feature to a confident diagnosis of CVT by CT or MR images.
Unfortunately,
these findings are not always evident,
and the diagnosis rests on nonfilling of a venous sinus or cortical vein.
(1)
-The primary sign of acute CVT on a non-contrast CT is hyperdensity of a cortical vein or dural sinus and are most clearly visualized when CT slices are perpendicular to the dural sinus or vein.
Thrombosis of the posterior portion of the superior sagittal sinus may appear as a dense triangle (the dense or filled delta sign).
(1,
8,
9)
- In contrast-enhanced imaging (CTV and MRV),
a well-described finding of sinus thrombosis consists in a central intraluminal filling defect representing a thrombus surrounded by contrast-enhanced dural collateral venous channels and cavernous spaces within the dural envelope (known as “empty delta sign”).
(1,
4,
8,
9) (Figure 4)
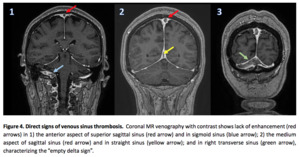
Fig. 3
- Unenhanced MR image is more sensitive for the detection of venous thrombi than is unenhanced CT.
The absence of a flow void and the presence of altered signal intensity in the sinus is a primary finding of sinus thrombosis on MRI.
However,
slow or turbulent flow also may cause a signal intensity alteration in the sinus,
which require a close assessment with multiple pulse sequences to avoid a misdiagnosis.
The administration of contrast material and the application of venographic techniques often are necessary for confident diagnosis. (4,
9)
- The signal intensity of venous thrombi on
T1- and T2-weighted MR image varies according to the interval between the onset of thrombus formation and the time of imaging,
with characteristic findings in each stage:
·
- Acute stage of thrombus formation (0-5 days): the signal is predominantly isointense on T1-weighted images (T1WI) and hypointense on T2-weighted images (T2WI) because of deoxyhemoglobin in red blood cells trapped in the thrombus.
The venous thrombus signal intensity in this stage may be very hypointense on T2- weighted images and may be mistakenly thought to indicate a flow void,
leading to diagnostic error.
Contrast-enhanced MR venography or CT venography is usually necessary to achieve a definitive diagnosis at this stage.
(1,
9)
- · Subacute stage of thrombus development (6 - 15 days): the signal is predominantly hyperintense on both T1-weighted images and T2-weighted images because of methemoglobin in the thrombus.
This stage of formation is the easiest stage at which to detect a thrombus on MR image,
as the signal intensity of the sinus is most different from that in normal flow states (increased signal intensity on both T1- weighted images and T2-weighted images is almost always abnormal.
(1,
9) (Fgure 5)
- · Chronic stage of thrombus development (> 15 days): the signal is typically isointense on T1-weighted images and isointense or hyperintense on T2-weighted images; however,
significant variability in thrombus signal intensity exists.
The signal intensity may be similar to that of very slow blood flow,
and on contrast MR images,
marked contrast enhancement may be observed that resembles the enhancement typically seen in a normal sinus.
This finding is presumably secondary to an organized thrombus with intrinsic vascularization as well as to slow flow in dural and intrathrombus collateral channels.
It is important to be aware that contrast enhancement of the sinus on MR images does not definitively indicate patency,
and venography usually is necessary for a definitive diagnosis.
(1,
9)
-Recanalization- During chronic thrombosed sinusus stages,
an irregular appearance of the sinus,
with multiple intrasinus channels and dural collateral vessels,
may be seen on MRV images and is characteristic of incomplete recanalization.
Complete recanalization may occur more often in thrombosis of the superior sagittal sinus and straight sinus than in thrombosis of the transverse and sigmoid sinuses after anticoagulation therapy,
though complete recanalization is not necessary for clinical recovery.
(9) (Figure 6)
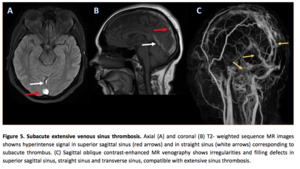
Fig. 4
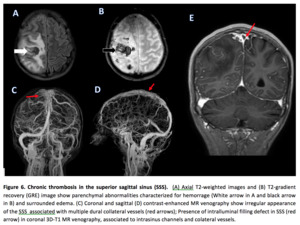
Fig. 5
# INDIRECT SIGNS OF THROMBOSIS
TYPICAL PARENCHYMAL ABNORMALITIES
-PARENCHYMAL SWELLING
- Diffuse cerebral swelling may be the only abnormality on CT and MR images in as many as 42% of patients with cerebral venous thrombosis,
and is characterized by sulcal effacement,
diminished cistern visibility,
and a reduction in ventricular size.
(9)
-Gyral swelling usually is the earliest sign of venous infarct,
which is often extremely subtle and only appreciable by noticing the effacement of the adjacent sulci.
(4)
-Patients with brain swelling and without parenchymal signal intensity changes tend to have intrasinus pressures in the intermediate range (20 - 25 mm Hg); although higher intrasinus pressures also may be reached.
(9,
14)
- It is typically reversible with therapy,
but can be lethal if not identified and treated appropriately.
CEREBRAL EDEMA
- Signal changes usually begin to occur when sinus pressures reach 32-42 mmHg.
(11)
- Imaging findings in edema should resolve over time if the primary cause is treated or adequate venous return pathways develop.
(14)
- Cerebral edema is best identifed on T2 or T2 FLAIR-weighted sequences,
which presents as T2 hyperintensity of the subcortical and periventricular white matter,
usually sparing the cerebral cortex.
(4)
- Diffused weighted MRI techniques allow subclassfication of parenchymal abnormalities as either primarily vasogenic edema (with increased ADC values) or primarily cytotoxic edema (with reduced ADC values).
(4,
8,
9)
- Venous infarction demonstrates as a low-attenuation lesion (with or without subcortical hemorrhage) that crosses usual arterial boundaries or are in close proximity to a venous sinus (1,
14) (Figure 7)
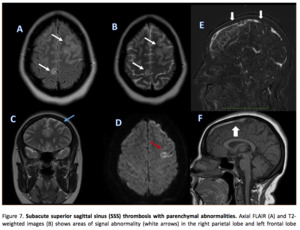
Fig. 6
- In contrast with arterial ischemic states,
many parenchymal abnormalities secondary to venous occlusion are reversible.
(8,
9,
11) But when marked diffusion restriction occurs,
particularly with associated parenchymal hemorrhage,
the risk of permanent imaging changes is much higher.
(9,
11)
- A relationship between the venous sinus occlusion site and the brain lesion site can be seen,
because the brain parenchymal lesions usually are related to a venous distribution.
(3,
8,
9,
12) (Table 2) (Figure 8)
|
SINUS AFFECTED
|
SUPERIOR SAGITTAL SINUS THROMBOSIS
|
TRANSVERSE AND SIGMOID SINUS THROMBOSIS
|
DEEP CEREBRAL VENOUS SYSTEM THROMBOSIS
|
|
PARENCHYMAL LESION LOCATION
|
-Parasagittal frontal,
parietal or occipital lesion;
(Irregularly and flame shape lobar hemorrhage)
|
- Inferior/posterior temporal lesion;
-Occipital lesion;
-Cerebellar parenchymal lesion
|
-Bilateral thalamic lesion
|
Table 2. Typically distribution of parenchymal changes based on affected venous sinus thrombosis.
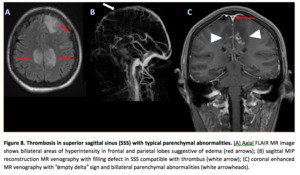
Fig. 7
HEMORRHAGE
- Parenchymal hemorrhage can be seen in one third of cases of cerebral venous thrombosis.
(9) Hemorrhagic complications are much more common in venous infarction,
than in arterial infarction,
whith microhemorrhage occurring in approximately 37% of venous infarcts and frank intracerebral hemorrhage (hemorrhage >1 cm) in about 21% of them.
Parenchymal hemorrhage correlates with high venous pressure (>42 mmHg) and is hypothesized to arise from venule rupture and infarction.
(5,
9)
- The mechanism of hemorrhage is multifactorial: 1) may be precipitated by continued arterial perfusion in areas of cell death (similar seen at reperfusion in arterial ischemia); 2) or caused by elevation of venous pressure beyond the limit of the venous wall,
with rupture of the hematoencephalic barrier due intravascular hypertension in the occluded territory.
(5,
9)
- Gradient-echo (GRE) and susceptibility-weighted imaging (SWI) allow for sensitive,
early detection of hemorrhage.
(5,
9)
- The distribution is typically cortical with subcortical extension,
and smaller zones of isolated subcortical hemorrhage also may be seen,
accompanied by minimal edema.
(4,
9)
-When a pattern of multiple structures of both superficial and deep venous systems of are involved there is probably a retrograde progression of the thrombus present in the superficial venous system.
(6)
IDIOPATHIC INTRACRANIAL HYPERTENSION
- Consist in a syndrome of increased intracranial pressure without an obvious explanation such as a mass lesion.
Symptoms and signs include headache,
nausea,
vomiting,
papilledema,
cranial nerve palsy,
and visual changes.
- Sinus thrombosis may occur as part of the intracranial hypertension syndrome and should be excluded with detailed imaging (MR imaging and MR venography or CT venography) in all pa- tients with such manifestations.
(9)
- Bilateral stenoses of the transverse sinuses,
without definitive evidence of current or prior thrombosis,
have been described in 93% of patients with idiopathic intracranial hypertension identified at MRV.
(9)
- Whether sinus stenoses are a cause or a result of increased intracranial pressure is a topic of ongoing study,
but there appears to be a dynamic relationship between cerebrospinal fluid pressure and venous sinus caliber.
(9)
#ATYPICAL PARENCHYMAL ABNORMALITIES
DEEP VENOUS OCCLUSION
- Thrombosis of the internal cerebral veins,
vein of Galen,
or straight sinus has been observed in approximately 16% of patients with cerebral venous thrombosis.
(9)
- Most such patients present with symptoms of elevated intracranial pressure that may rapidly escalate to a coma.
(9)
- The main signs of deep venous system thrombosis are due to the localization of the secondary parenchymal manifestations.
(5)
- Thalamic edema is the imaging hallmark of this condition (seen in 76% of CT and 86% of MR studies),
and it may extend into the caudate regions,
basal nuclei,
deep white matter,
the superior portion of the cerebellum and mesencephalon.
(5,
8,
9)
- Thalamic parenchymal abnormalities are usually bilateral and have a triangular shape that is specific for venous stroke.
(15) Unilateral thalamic edema may occur but is rare (FIGURE).
(7,
8,
9)
- Hemorrhage is noted in 19% of patients and typically is located in the thalami.
(8,
9) (Figure 9)
- Despite its extensive nature,
if the edema is primarily vasogenic (with elevated ADC values),
it may resolve without sequelae.
(9)
- The lack of flow-void in the deep venous system is very suggestive for a venous thrombosis.
(8)
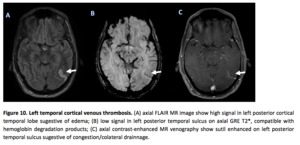
Fig. 9
ISOLATED CORTICAL VENOUS THROMBOSIS
-Isolated cortical venous thrombosis is a relatively rare entity.
(8,
9)
- Typical parenchymal findings are areas of focal cortical edema or hemorrhage,
which may be nonspecific.
(9) (Figures 10 and 11)
- The finding of an adjacent thrombosed venous structure is the the most specific sign of this disorder,
and has been referred to as the “cord sign”on CT studies; on MR images,
it has been called the “hyperintense vein sign”.
(1,
8,
9)
- MRV may show an asymmetric absence of flow signal or diminished enhancement in the thrombosed cortical veins.
Evaluation of the MR venographic source images is typically necessary to make this determination.
(9)
- It is particularly difficult to diagnose by using only T1WI,
T2WI,
and MRV imaging for several reasons: cortical veins are extremely variable in number,
size,
and location; occluded small veins at the cortical level are difficult to identify by using these MRI sequencies; and only the occlusion of the largest veins is detectable on MRV.
GRE images can play a important role in evaluation of these thrombus.
(8) (Figure 12)
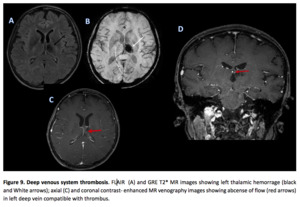
Fig. 8
SUBARACHNOID HEMORRHAGE (SAH)
-Is a rare clinical presentation when secondary to CVT,
but could be potentially life-threatening because it can lead to strokes in young adults (4).







