Entamoeba histolytica
Entamoeba histolytica is responsible for amebiasis.
It is believed that 1% of the world's population is infected -> and up to 100,000 related deaths are reported annually
Infection is more frequent among the lower socio-economic classes in tropical and subtropical climates:
- Immigrants from endemic areas
- Institutionalized populations (for example,
those with mental retardation)
- Overcrowding
- homosexual promiscuous men
The majority of severe cases have been identified among newborns,
during pregnancy and postpartum,
the use of corticosteroids,
malignancy and malnutrition.
Thoracic disease is the second most frequent manifestation of extraintestinal amoebiasis
7-20% of all cases of liver disease -> 2% of patients with intestinal disease.
Thoracic infection can result in several ways:
- Direct extension of a hepatic abscess to the thorax,
which occurs in 6-40% of patients with liver involvement
- Hematogenous spread; and rarely,
the aspiration
Fig. 1
Pericardial involvement is present in less than 2% of all thoracic complications
Pain,
cardiac tamponade and sepsis are the most common clinical findings
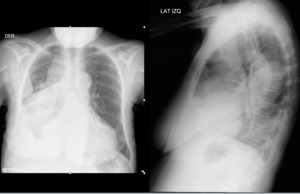
Fig. 2: Patient of 59 years. Right abdominal thorax pain associated with fever. Chest x-ray shows right pleural effusion in moderate amount.

Fig. 3: Contrast thorax tomography: patient figure 2, coronal images showing hepatic abscess associated with complicated right pleural effusion.
Malaria
The parasite is transmitted by the Anopheles mosquito.
Merozoites develop from schizonts within erythrocytes and are released by hemolysis at different time intervals depending on the species.
Between 400 and 490 million people are infected,
and about 2.2–2.5 million deaths result annually worldwide in endemic areas such as South America,
Africa,
and southern Asia.
Fever with chills,
sweating,
anemia,
leucopenia,
and splenomegaly are the most common clinical findings.
The diagnosis is usually made by identifying trophozoites or other parasitic forms within the erythrocytes in a thin blood smear or parasites in a thick smear.
Serologic and nucleic acid amplification tests are also available.
Adult respiratory distress syndrome (ARDS) is the primary manifestation of malaria in the lung and was included in 1990 by the World Health Organization as a criterion for the definition of both severe and complicated malaria.
Although the pathophysiologic features of ARDS are still unclear,
changes result from vascular injury related to red blood cell sequestration and destruction,
the release of parasite and erythrocyte material into the circulation,
and the host response to these events.
Severe P falciparum infection is the type most commonly associated with ARDS,
but cases caused by P vivax and P ovale have also been reported.
Radiographic and CT findings are consistent with noncardiogenic pulmonary edema.
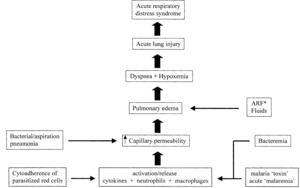
Fig. 4: Acute respiratory distress syndrome in malaria.

Fig. 5: Acute respiratory distress syndrome (ARDS) in a young patient with P. falciparum malaria. PA chest x-ray demonstrates bilateral and heterogeneous use of opacities in all four quadrants of the lungs. Other clinical criteria for ARDS were positive. Parasitic forms of P. falciparum were identified in the thin peripheral blood smear
Trypanosomiasis
Trypanosoma cruzi is the etiological agent of American trypanosomiasis or Chagas disease.
The infection is acquired through the bite of an insect of the family Reduviidae (genera Triatoma,
Rhodnius and Panstrongylus),
through the inoculation of trypomastigotes in the human body.
The insect usually defecates near the bite and inoculation can occur when rubbing the insect's stool over the bite or some other skin defect
Chagas disease is endemic to areas of Central and South America,
especially Argentina,
Brazil,
Bolivia,
Chile,
Paraguay and Uruguay.
In 2000,
WHO estimated that between 16 and 18 million people were infected in American countries.
Around 45,000 people die annually due to the disease.
Chagas disease has also been described in the southwestern United States among immigrants from endemic areas.
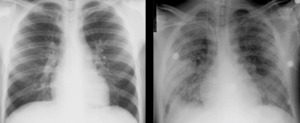
Fig. 6: PA chest radiography essentially normal in a patient with diffuse adenopathy, fever and weakness. PA chest x-ray 48 h later shows the development of parenchymal opacities of compatible use with pulmonary edema. The patient eventually developed ventricular tachyarrhythmia and died.
Cardiac MRI in Chagas disease:
The areas of myocardial fibrosis are identified as late myocardial enhancement (10-20 minutes) in the IR-echo gradient sequences.
These hyperintense areas,
which may be transmural,
subendocardial,
along the medial wall,
and subepicardial,
are more likely to be identified toward the apex walls,
inferior and inferolateral.
Gravity marker among seropositive patients,
especially those who are asymptomatic
Toxoplasmosis
Toxoplasma gondii infection - an intracellular protozoan found in a variety of animals such as birds and humans - the last reservoir is feline
Affected individuals have a cell-mediated immunodeficiency such as AIDS,
usually with a CD4 count of less than 200 / mm3.
Infection is acquired through the ingestion of contaminated food or drinks or tissue-shaped meat from intermediate hosts.
Transplacental infection is also a well known pathway that results in congenital toxoplasmosis.
The lungs and the heart are the most frequently affected organs after the central nervous system
The lung can be affected primarily or as a result of the spread of a CNS infection.
Clinical manifestations of Toxoplasma pneumonia include fever,
cough and dyspnea; however,
it may be asymptomatic or minimally symptomatic.
Myocardial involvement includes arrhythmias (atrial and ventricular),
sudden death,
AV block,
pericarditis and heart failure.
Diagnosis is usually made by identifying parasites in bronchoalveolar lavage and lung biopsy or cardiac tissues of patients with acute myocarditis
Ascaris
The infection with Ascaris lumbricoides = is among the most frequent parasitic infections worldwide.
It is believed that human infection is present in a quarter of the world population.
with an estimated mortality between 20,000 and 60,000 per year,
mainly as a result of an intestinal infection obstruction.
The parasite has a worldwide distribution; however,
tropical and subtropical climates in Southeast Asia,
Africa and Central and South America
Asymptomatic,
up to 15% of infected patients may experience clinical symptoms.
Lung disease is usually asymptomatic,
but up to 20% of patients will present with fever,
cough,
expectoration and eosinophilia in peripheral blood,
sometimes recognized as Loefler's-like syndrome.
Asthma has also been described in the context of ascariasis.
Eosinophils and Charcot-Leyden crystals are identified in the sputum.
Confirmation requires identification of larvae in sputum or gastric aspirates
In patients from non-endemic areas with pulmonary symptoms,
diagnosis is suggested when eggs are present in the feces.
Chest X-rays and CT scans may show migratory,
frosted glass and alveolar opacities that typically clear up within days or weeks (lobar consolidation and alveolar hemorrhage have also been described.
Larva Migrans Visceral - Loeffler's syndrome
Visceral larva migrans or Loeffler syndrome,
is an infection classically caused by Toxocara canis and Toxocara catis; however,
the association with Ascaris suum has also been described.
In all three species,
the infection is usually acquired by ingestion of contaminated products
VLM due to T.
canis and T.
catis can cause lung disease in 25-85%.
Wheezing -> severe bronchiolitis,
asthma,
and acute / chronic eosinophilic pneumonia with respiratory failure,
usually with associated peripheral blood eosinophilia.
The pulmonary migration of A.
suum triggers an inflammatory reaction similar to that provoked by A.
lumbricoides.
The clinical forms of infection with A.
suum are similar to other presentations of VLM.
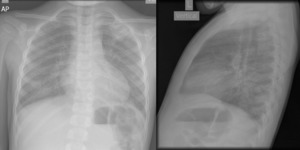
Fig. 7: Chest x-ray: bilateral reticular opacities with nodular images in left upper lobe and right retrocardia.

Fig. 8: Chest tomography: consolidations in the left superior lobe and right retrocardia.
Diagnosis: detection of antibodies by the enzyme linked immunosorbent assay (ELISA).
The larvae of A.
suum can be isolated in respiratory secretions and gastric aspirations during the pulmonary phase.
Strongyloides
Humans are the main host of the microscopic nematode Strongyloides stercoralis
Although the reports on the global prevalence of the disease are very different (from 1 to 100 million people worldwide).
It seems clear that strongyloidiasis is not as frequent as infection with other nematodes (eg,
Ascaris lumbricoides or Trichuris trichiura).
The parasite is found in all tropical and subtropical regions
Continuous autoinfection,
which can lead to a massive and potentially fatal parasitic infestation (the so-called hyperinfection syndrome),
especially in patients with AIDS and in patients receiving glucocorticoid therapy.
Hyperinfection syndrome is associated with a mortality rate close to 100% without treatment and perhaps more than 25% when treated.
The definitive diagnosis is made by identifying larvae in the sputum,
bronchoalveolar lavage or lung biopsy
Echinococcus
At least four species of Echinococcus can infect humans:
- E.
granulosus,
- E.
multilocularis,
- E.
vogeli
- E.
oligarthrus.
The infection is acquired by eating food / drinks contaminated with eggs.
The larvae penetrate the intestinal wall and migrate mainly to the liver.
E.
granulosus,
the most common Echinococcus to cause disease,
is seen in the Mediterranean region,
Eastern Europe,
Africa,
South America.
Unilocular cystic echinococcosis is caused by E.
granulosus.
In general,
the liver is the most commonly affected organ; however,
thoracic disease is a very common presentation among adults and perhaps the most common among children.
Various organs in the thorax can be affected by the disease,
either by the growth of liver cysts that pass through the diaphragm or by hematogenous spread.
Although the lungs are affected in most cases of thoracic hydatid disease,
other thoracic organs may be pleural sutures,
parietal pleura,
chest wall,
mediastinum,
diaphragm,
and heart.
Pathologically,
the cysts consist of three layers:
- 1.
The pericyte,
composed of fibroblasts,
giant cells and eosinophils,
which form a rigid layer
- 2.
An acellular membrane of medium laminate with nutritional functions
- 3.
A thin,
translucent inner germ layer that contains several scolices and generates daughter cysts.
Cystic = solitary (60% of cases) or multiple,
unilateral or bilateral (20-50%).
The lesions are identified predominantly in the lower lobes (60%) and can exhibit diameters between 1 and 20 cm.
The coexistence of liver and lung disease is present in only 6% of patients.
The uncomplicated cysts,
the most common presentation,
can be seen as round or oval masses that have well defined edges,
do not enhance with the injection of contrast material,
while the pericism enhances if it is infected and has a hypoatenuating content with respect to the capsule.
In magnetic resonance,
the cyst content appears characteristically hypointense in T1 and hyperintense in T2-weighted images with a well-defined wall that is isointense and hypostense respectively.
The development of cysts in the mother's cyst is an early sign of degeneration.
In MRI,
the content of the mother's cyst tends to be more intense with viable hyposynthetic cysts in T1 and both cysts are isointense in the T2-weighted images.
The "meniscus sign" or "crescent sign",
which is characterized by the presence of air between the periciste and the laminated membrane,
appears as the growth continues and the cysts erode the adjacent bronchioles.
It is considered to be a sign of impending breakdown.
The cystic rupture can give rise to different radiological signs.
e "double arch",
"cumbo sign" or "sign of onion peel",
defined as the presence of the meniscus sign and an air level within the endocyst.
e "water lily sign" represents an endocyst floats in a partially hidden cyst
Paragonimiasis
Ingestion of raw or partially cooked freshwater crabs containing Paragonimus westermani (lung flea) or other Paragonimus species.
Alternatively,
undercooked meat from infected pigs and wild boar are also sources.
The infection is endemic in areas of East Asia,
Southeast Asia,
Latin America and Africa.
Many cases have been reported in the United States between Indochinese and Latin American immigrants It is believed that there are 195 million people at risk and 20.7 million are infected in endemic areas
Radiologic findings correlate well with the stage of the disease.
The penetration of juvenile worms through the diaphragm into the pleural cavity can cause pleural effusion or pneumothorax.
Once the parasites get to the lung,
patchy airspace consolidation can occur,
a phenomenon that reflects the presence of an exudative or hemorrhagic pneumonia which can cavitate.
Contrast materia enhanced CT performed during this stage may show hypoattenuating fluid-filled cysts surrounded by hyperattenuating consolidation in the adjacent lung.
Linear areas of increased opacity or hyperattenuation indicate peripheral atelectasis or worm migration.
Worm cysts,
whose diameters range from 0.5 to 1.5 cm,
are better visualized after the consolidation resolves and manifest as either solitary or multiple nodules communication with the airway.
Chest radiographic and CT findings include a ring shadow usually less than 3 mm thick and a crescent-shaped area of increased opacity or hyperattenuation within the cyst that represents worms attached to the wall.
Complications of cysts include pleural effusion,
empyema,
and pneumothorax.
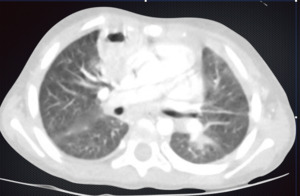
Fig. 9: Chest tomography with cavern in lower right lobe and frosted glass opacities.
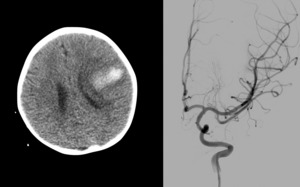
Fig. 10: Simple cranial tomography: left frontal intraparenchymal hemorrhage. Cerebral arteriography: lesion type infectious aneurysm is observed.





 in a young patient with P. falciparum malaria. PA chest x-ray demonstrates bilateral and heterogeneous use of opacities in all four quadrants of the lungs. Other clinical criteria for ARDS were positive. Parasitic forms of P. falciparum were identified in the thin peripheral blood smear")




