THE ROLE OF MRI
MRI quite adequately complements findings from other diagnostic tools such as muscle biopsy and electromyography,
which may not be decisive for establishing a final diagnosis in patients with overlapping findings or non-specific clinical phenotypes and together may hint at a smaller number of possible conditions.
In general,
muscle MRI has a higher diagnostic yield in slowly progressive diseases in which selective patterns of muscle involvement can be discerned through a prolonged period of time.
Mild,
episodic or extensive and severe involvement does not allow for a clear pattern detection and poses difficulties for MRI interpretation.
Muscle imaging is less relevant in DMD/BMD,
FSHD and DM,
since they can be readily diagnosed on clinical and histopathological grounds.
Fig. 62
CONVENTIONAL MRI PROTOCOLS
Our presentation focuses on the usage of conventional MRI for morphological evaluation of suspected myopathies.
At our institution,
a whole-body MRI scan with axial T1WI is performed in suspected inherited myopathy and additional whole-body axial STIR sequences are included if an acquired myopathy or inflammatory changes are suspected.
The following table summarises the main protocols recommended in the literature.

Fig. 9
The value of additional contrast imaging remains controversial,
and it has not been proven to provide additional information compared to STIR / T2 FS sequences.
MRI FINDINGS
Regarding the pathological findings described in the background of this presentation,
they show distinct MRI features,
which are summarized in Fig.
below.
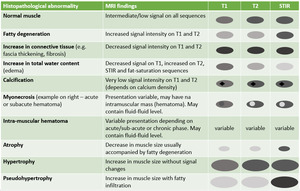
Fig. 11
Some examples are presented below regarding the major MRI findings.
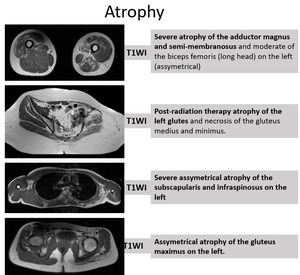
Fig. 12
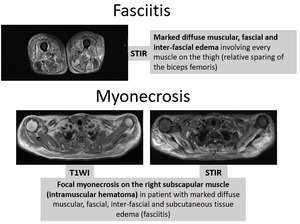
Fig. 13
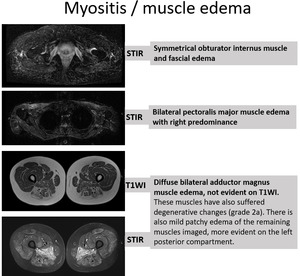
Fig. 14
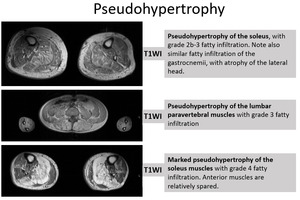
Fig. 15
Some aspects of muscle fatty infiltration require particular attention,
such as involvement of specific compartments,
fatty infiltration patterns of affected muscles and the corresponding negative,
i.
e.,
muscle sparing.
Below are some examples:
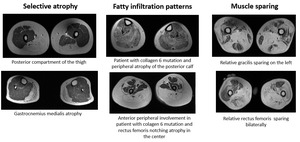
Fig. 56
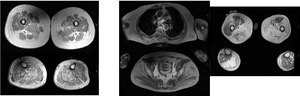
Fig. 57: Two patients with lower-limb girdle myopathy. Note marked involvement of the pelvis and proximal lower limbs.
MRI SCALES FOR DYSTROPHIC CHANGES
There are several well-established rating scales on MRI concerning the visual rating of dystrophic change of striated muscle tissue.
The most commonly used has been described by Mercuri et al in 2002.
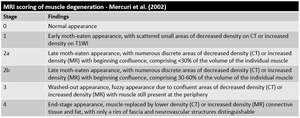
Fig. 10: Note: These scales do not refer to "atrophy", i.e., reduction in muscle size. Although fatty infiltration is expected to be present in an atrophic muscle, the contrary may not be true (for instance, pseudohypertrophy increases muscle size). However these terms are used interchangeably in the literature, tey might render distinct clinical features or severity of symptoms.
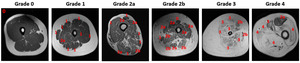
Fig. 16: Fatty infiltration grading acording to Mercuri et al.
CLINICAL CASES
Case 1 - Patient with Pompe disease
33 years old patient with diagnosis of Pompe disease.
There is paravertebral involvement with cranio-caudal gradient (red arrows),
discrete atrophy of latissimus dorsi and asymmetric fatty infiltration of the abdominal wall muscles (blue arrow).
On the images below,
you can also see gluteus minimus and medius atrophy (grade 2-3).
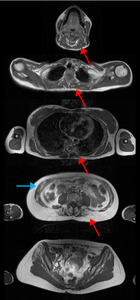
Fig. 17: Cranio-caudal progressive para-vertebral atrophy with lumbar involvement grade 3-4 (red arrows).
Discrete atrophy of latissimus dorsi.
Fatty infiltration of the anterior abdominal wall muscles (blue arrow).
Gluteus minimus and medius grade 2-3 atrophy.
Figure below shows leg involvement with volumetric reduction of the adductor magnus,
fatty infiltration of the hamstrings and mild muscle edema / myositis of the posterior thigh with sparing of semitendinosus (blue arrwos) and the distal leg.
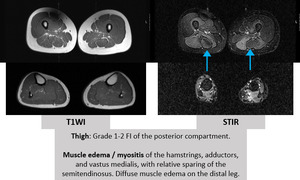
Fig. 18: Edema sparing of the semitendinosus (blue arrows).
Case 2 - Centronuclear myopathy
The following patient,
44 years old,
was being studied for a hereditary myopathy.
WBMRI seen on Fig.
shows posterior thigh involvement with grade 1-2 fatty infiltration (blue brackets) and severe (grade 4) selective gastrocnemius medialis involvement on the legs (red arrows).
Patient also had moderate deltoid fatty infiltration and paravertebral dorsal and lumbar involvement.
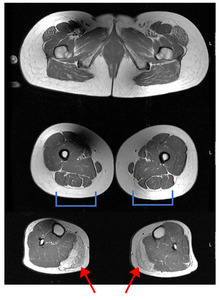
Fig. 19: Tensor fasciae lateae and gluteus maximus involvement (grade 2).
Mild hamstring and quadricipital involvement, more pronounced on the posteroir compartment (blue arrows).
Severe (grade 4) gastrocnemius medialis involvement (red arrows)
Case 3 - Suspected congenital myopathy
50 year-old patient with clinically evident muscle atrophy,
particularly of the upper limb-girdle and hands,
with difficulty performing daily tasks and walking.
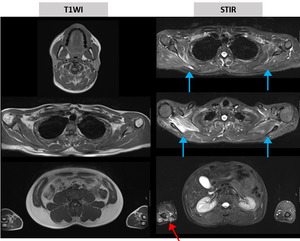
Fig. 20: Assymetrical edema of the upper limb girdle, affecting the rotator cuff (more prominent on the right, blue arrows)
Lower limb girdle relatively spared
Arm muscle edema (red arrow).
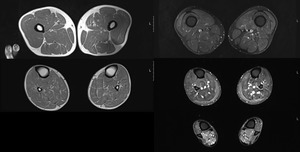
Fig. 21: Sartorius and adductor fatty infiltration grade 1.
Mild involvement of the hamstrings and quadriceps (symmetrical).
Mild involvement of the gastrocnemii and soleus.
Assymetrical muscle edema of the gastrocnemius medialis on the left.
Symmetric muscle edema of the distal lower leg muscles.
Vastus medialis and semimembranosus edema, bilateraly.
Case 4 - Pompe disease
29 years-old patient with long-standing paresia which started during infancy.
Pompe disease has been confirmed.
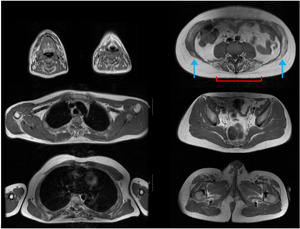
Fig. 22: Oral cavity and tongue with grade 1-2 fatty infiltration.
Right Subscapularis grade 1-2, deltoid grade 1.
Para-vertebral grade 2-3, with cranio-caudal severity.
Anterior abdominal wall muscles grade 2-3.
Iliopsoas atrophy grade 1.
Sartorius and hamstrings atrophy grade 1.
Adductors grade 2-3 on the right and rectus femoris grade 3, bilaterally
Soleus grade 1.
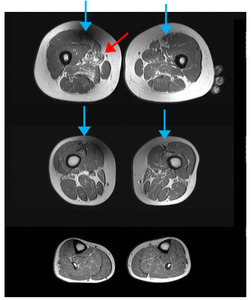
Fig. 23: Sartorius and hamstrings atrophy grade 1
Adductors grade 2-3 on the right and rectus femoris atrophy grade 3, bilaterally
Soleus atrophy grade 1.
Case 5 - Patient with Inclusion body myositis
17 year-old patient with biopsy-confirmed inclusion body myositis.
Note the asymmetric distribution with important degenerative changes and only mild inflammatory findings.
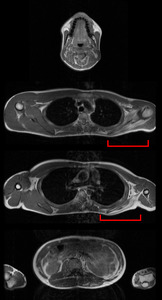
Fig. 24: Assymetric involvement of the trapezius, deltoid and rotator cuff with relative preservation on the right (red brackets).
Triceps brachialis atrophy grade 1.
Atrophy of the rhomboids and latissimus dorsi.
Multifidus atrophy on the left.
Atrophy of the anterior abdominal wall muscles.
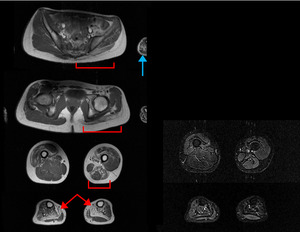
Fig. 25: Grade 3 atrophy of the iliopsoas.
Fatty infiltration and atrophy of the gluteus maximus, obturators and piriformis.
Assymetric atrophy of the quadriceps, adductors and hamstrings
Quadriceps myositis.
Grade 4 soleus, grade 1-2 tibialis anterior, grade 1 gastrocnemius medialis.
Case 6 - Ullrich myopathy
16 year-old patient with collagen 6 gene mutation (COL6A2),
presenting with upper and lower limb-girdle paresia.
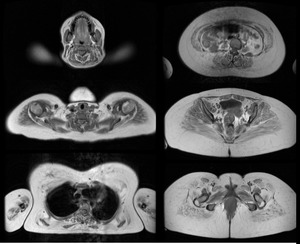
Fig. 26: Marked fatty infiltration of the trapezius, rotator cuff and pectorals, anterior abdominal wall muscles, gluteus and anterior thigh
Posterior thigh
Posterior lower leg more affected than the anterior compartment
Paravertebral muscles relatively preserved by comparison
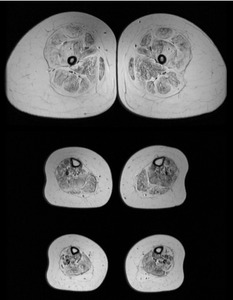
Fig. 27: Marked fatty infiltration of the trapezius, rotator cuff and pectorals, anterior abdominal wall muscles, gluteus and anterior thigh
Posterior thigh
Posterior lower leg more affected than the anterior compartment
Paravertebral muscles relatively preserved by comparsison
Case 7 - Dermatomyositis
4 years-old patient with 1-week onset of reduced activity during the day,
low fever spikes,
astenia,
reduced appetite,
facial erithema and myalgias during gait,
especially when climbing stairs.
Thre is also reduced upper limb strength.
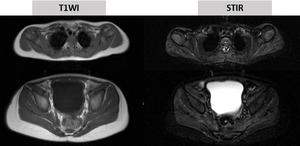
Fig. 28: Marked fatty infiltration of the trapezius, rotator cuff and pectorals, anterior abdominal wall muscles, gluteus and anterior thigh
Posterior thigh
Posterior lower leg more affected than the anterior compartment
Paravertebral muscles relatively preserved by comparsison
Fig. 29: Marked fatty infiltration of the trapezius, rotator cuff and pectorals, anterior abdominal wall muscles, gluteus and anterior thigh
Posterior thigh
Posterior lower leg more affected than the anterior compartment
Paravertebral muscles relatively preserved by comparsison
Case 8 - Polymyositis
39 years-old patient with myopathic symptoms with asymmetric proximal paresia and muscular atrophy.
Relevant paresia during neck flexion.
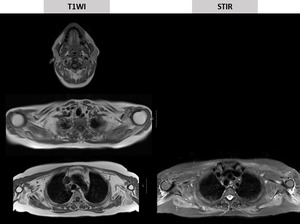
Fig. 30: Diffuse scapular muscle atrophy with relative preservation of the trapezius.
Trunk and paravertebral muscle atrophy grade 1-2
Upper limb-girdle muscle edema involving the rotator cuff.
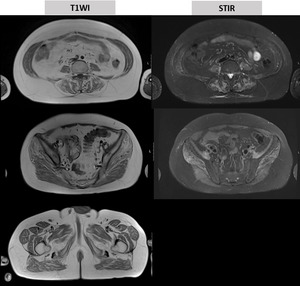
Fig. 31: Diffuse atrophy of the lower limb-girdle, involving the glutes (grade 2).
Diffuse limb-girdle edema also involving the adductors, and paravertebral muscles.
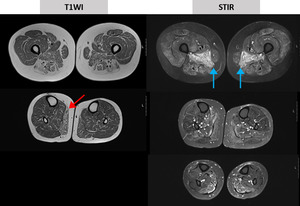
Fig. 32: Lower limb diffuse grade 2 muscle atrophy with edema predominantly affecting the gastrocnemius medialis
Marked edema of the adductor magnus (blue arrows).
Case 9 - Facio-scapulo-humeral / facio-scapulo-peroneal dystrophy
13 years-old patient with facio-scapulo-humeral dystrophy,
presenting with facial diplegia,
limb-girdle paresia,
scoliosis,
respiratory insufficiency and severe hearing loss.

Fig. 33: Sternocleidomastoid muscle volume reduction, symmetrical.
Trapezius muscle fatty infiltration grade 3 and 4 on the left.
Assymetrical deltoid muscle atrophy, grade 3-4.
Pectorals, latissimus dorsia and rhomboid severe involvement.
Cervico-dorsal paravertebral muscle involvement with multifidus atrophy.
Triceps grade 3-4 atrophy.
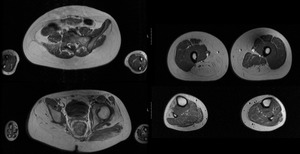
Fig. 34:
Rectus abdominis grade 4 atrophy.
Iliopsoas grade 2 atrophy on the right
Right gluteus muscles atrophy grade 3-4.
Right rectus femoris grade 2 atrophy.
Grade 4 vastus medialis atrophy, asymmetrical adductor involvement.
Hamstring near-total fatty infiltration.
Tibial anterior and peroneal grade 4.
Case 10 - LGMD - suspected calpainopathy
63 year-old patient presenting with complaints of lower limb-girdle weakness with onset during first decade of life.
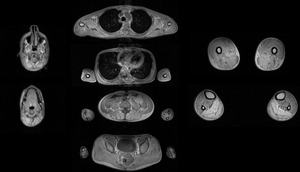
Fig. 1: LGMD - suspected calpainopathy.WBMRI shows symmetrical affection of the soleus and gastrocnemius, with severe fatty infiltration (grade 4), without significant atrophy or pseudohypertrophy. There is aductor longus grade 4 atrophy, adductor magnus and hamstrings grade 2 and grade 3 on the right and left, respectively.
Lumbar paraspinalis grade 3 atrophy.
Increased myocardium signal, suggestive of fatty infiltration.
The pterigoyd muscles and the tongue as well as the mouth pavement muscles are moderately involved.
Cervical paravertebral muscles are moderately involved.
In the shoulder, the rotator cuff muscles are also moderately involved.
In the lower limb-girdle, the iliopsoas, lumbar paravertebral muscles and glutes are moderately involved.
Case 11 - Necrotizing myositis
52 years-old patient with 4-week onset of subutaneous edema starting in the hands and progressing to the lower limbs and peri-orbital tissue,
accompanied by generalized myalgia.
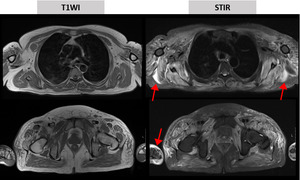
Fig. 35: Extensive muscle edema / myositis and peri-fascial edema (red arrows), as well as subcutaneous edema (blue arrow).
There is no specific pattern, as the edema is diffuse along the whole body.
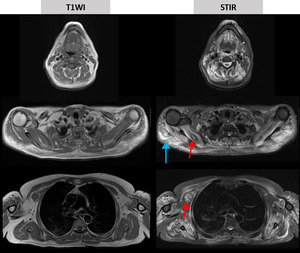
Fig. 36: Extensive muscle edema / myositis and peri-fascial edema, as well as subcutaneous edema (blue arrow).
There is no specific pattern, as the edema is diffuse along the whole body. You can notice foci of muscle necrosis (red arrows) on the subscapularis on the right and pectoralis minor also on the right.
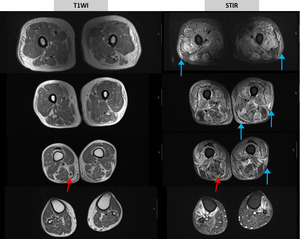
Fig. 37: Extensive muscle edema / myositis and peri-fascial edema, as well as subcutaneous edema (blue arrow).
There is no specific pattern, as the edema is diffuse along the whole body.
On the posterior thigh, there is evidence of muscle atrophy (red arrows).







Lower limb girdle relatively spared
Arm muscle edema (red arrow).")
.
Mild involvement of the gastrocnemii and soleus.
Assymetrical muscle edema of the gastrocnemius medialis on the left.
Symmetric muscle edema of the distal lower leg muscles.
Vastus medialis and semimembranosus edema, bilateraly.")