Etiologic agent and pathogenesis
Paracoccidioidomycosis is caused by Paracoccidioides brasiliensis and Paracoccidioides lutzii,
thermally dimorphic fungi believed to be soil saprophytes.
In its mycelial form,
Paracoccidioides spp produces infectious propagules known as microconidia that reach the alveoli after being inhaled; once in the lungs,
they interact with pulmonary macrophages and convert into a yeast form [1].
The latter form produces the appearance typically described in histopathological studies as a “pilot’s wheel”,
consisting of a mother cell surrounded by multiple blastoconidia (Fig.
1).
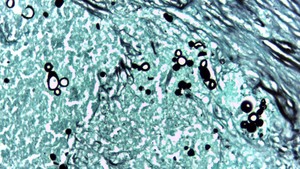
Fig. 1: Photomicrograph (original magnification, ×40; Grocott-Gomori methenamine–silver nitrate stain) shows the typical round form of P brasiliensis with multiple budding daughter cells.
References: Department of Pathology, Clínica CES/ Medellín 2017
The infection usually produces an inflammatory response that blocks fungal growth and yeasts may remain quiescent within granulomas without ever causing any symptoms.
However,
in conditions of immune imbalance,
the infection may progress to overt pulmonary disease and even spread to organs such as the liver,
adrenal glands,
kidneys,
spleen,
brain,
etcetera.
The minority of cases can present with systemic disease in the absence of a latency period,
having a rapid and aggressive clinical course [2].
Epidemiology
Although classically considered a disease geographically restricted to Latin America,
particularly Brazil,
Colombia,
Venezuela and Argentina,
paracoccidioidomycosis has been reported in North America,
Europe and Asia from patients who have previously lived in endemic areas.
Within these areas,
the infection is found in regions with some ecological factors like high precipitation rates,
tropical or subtropical forests and temperatures between 17 and 24 °C [3].
There is a clear male predominance with a male to female ratio of 13:1 among adults,
partially attributed to the inhibitory effects of ß-estradiol on the mycelial to yeast transformation.
This fact also explains the similar incidence of the disease between prepubescent males and females [1].
Most patients are 30 to 60 years old and more than 70% have worked in agricultural jobs.
Epidemiological data based on paracoccidin intradermal test reveal that up to 50-75% of people living in endemic areas have been exposed to Paracoccidioides spp,
but only 2 % develop the disease [4].
Clinical course
Around 90% of paracoccidioidomycosis cases correspond to a chronic or adult form,
generally resulting from reactivation of pulmonary latent foci.
Although lungs are the primary target of this infection,
some patients may be asymptomatic initially,
posteriorly developing nonspecific manifestations including cough,
shortness of breath,
prolonged fever and weight loss; notably,
many patients seek medical attention because of symptoms related to disseminated disease instead of those associated with pulmonary involvement.
Multifocal disease occurs in approximately 75%,
compromising the oropharyngeal mucosa in half of patients and sometimes extending to the nasal cavity,
lips and larynx [4].
Other organs commonly affected are the adrenal glands,
potentially leading to Addison’s disease in up to 3% [5]; spleen and liver involvement can also be seen,
as well as brain,
skin and bone lesions,
especially the shoulder girdle.
The other side of the spectrum of paracoccidioidomycosis is the acute or juvenile form,
representing less than 10% of cases. This presentation of the disease mainly affects the reticuloendothelial system,
thus producing hepatosplenomegaly,
lymphadenopathy and bone marrow dysfunction; unlike the chronic form,
lung involvement is rarely evidenced (both clinically and radiologically) at the time of diagnosis.
It has a more rapid progression with high mortality rates if left untreated and patients are almost always less than 30 years.

 shows the typical round form of P brasiliensis with multiple budding daughter cells. References: Department of Pathology, Clínica CES/ Medellín 2017")