ECR 2018 / C-3222
Pulmonary paracoccidioidomycosis: an imaging dilemma.
Congress:
ECR 2018
Poster Number:
C-3222
Type:
Educational Exhibit
Keywords:
Thorax, Lung, CT, Conventional radiography, Education, Biopsy, Infection, Occupational / Environmental hazards
Authors:
J. Reina1, M. F. Saldarriaga2, A. T. suarez1; 1Medellin/CO, 2Medellin, Antioquia/CO
DOI:
10.1594/ecr2018/C-3222
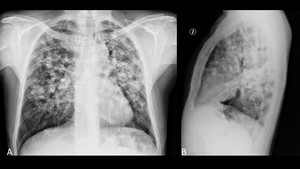
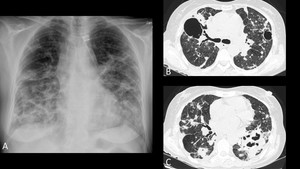
 and lateral (B) views. Bilateral ill-defined nodules along with reticular opacities predominantly in middle and upper lung zones. References: Department of Radiology, Clínica Universitaria Bolivariana / Medellín 2017")
Fig. 2:
Chest plain radiograph.Frontal (A) and lateral (B) views. Bilateral ill-defined...
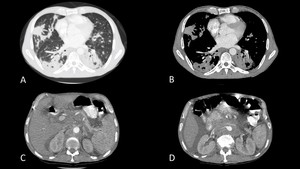
 and soft tissue windows (B) depicting irregular airspace consolidations involving both lungs. Contrast enhanced CT of the abdomen in the same patient (C and D) demonstrating spleen infiltration as well as retroperitoneal lymph node enlargement. References: Department of Radiology, Hospital Universitario San Vicente Fundación / Medellín 2017")
Fig. 3:
Chronic paracoccidioidomycosis in a 42-year-old male. Contrast enhanced CT of...
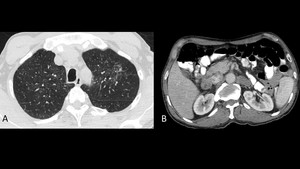
 showing subtle ground glass opacities in both upper lobes. Contrast enhanced CT of the abdomen (B) with evidence of a 26mm mass in the right adrenal gland and a 33mm mass in the contralateral gland. References: Department of Radiology, Hospital Universitario San Vicente Fundación / Medellín 2017")
Fig. 4:
63-year-old male with Addison’s disease secondary to chronic...

Fig. 5:
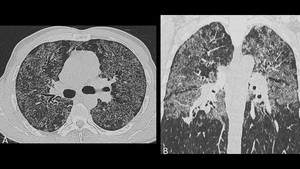
53-year-old patient who had previously worked in a cotton plantation. Chest...
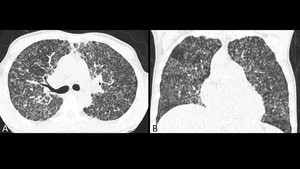
 and coronal (B) planes confirming the presence of miliary nodules resembling tuberculosis. References: Department of Radiology, Hospital Universitario San Vicente Fundación / Medellín 2017")
Fig. 6:
Same patient as in figure 5. High resolution CT in axial (A) and coronal (B)...

Fig. 7:
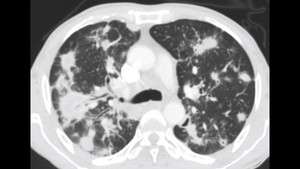
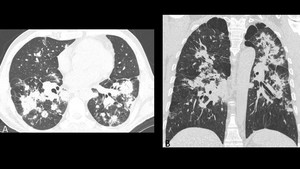
Male rural worker with chronic paraccocidioidomycosis. Contrast enhanced CT in...
 depicts bilateral areas of airspace consolidation, fibrotic changes and some cavitations. High resolution CT (B and C) better illustrates the architectural distorsion and cavitations associated to chronic paracoccidioidomycosis. References: Department of Radiology, Hospital Universitario San Vicente Fundación / Medellín 2016")
Fig. 8:
49-year-old female with 10 months of cough, occasional hemoptysis, weight loss...
")
Fig. 9:
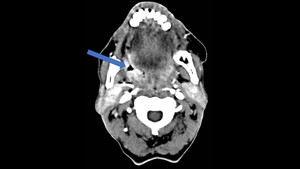
45-year-old rural worker with an ulcer in the oropharynx. A previous biopsy ...
 and coronal (B) planes demonstrating multiple random and confluent micronodules in both lungs. The patient was initially misdiagnosed as having an oropharyngeal cancer with pulmonary dissemination and posteriorly went into surgery. The histopathological analysis of the surgical specimen ruled out malignancy and confirmed paracoccidioidomycosis.")
Fig. 10:
Same patient as in figure 9. High resolution CT in axial (A) and coronal (B)...
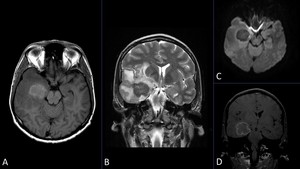
 and markedly hypointense in T2 WI (B);it presents peripheral enhancement after the injection of contrast agent (C) but there is no diffusion restriction (D). Note the midline deviation and uncal herniation. References: CediMed / Medellín 2017")
Fig. 11:
51-year-old male with headache and dizziness in the last year. MR images show a...
 and coronal (B) images. Multiple coalescing nodules with random distribution are visualized in both lungs; some of these nodules present spiculated borders and ground glass halo and are accompanied of interlobular septal thickening as well as paraseptal emphysema.")
Fig. 12:
Chest CT corresponding to the same patient in figure 11. Axial (A) and coronal...