ECR 2019 / C-0183
Keys for diagnosis of intracranial pressure disorders
Congress:
ECR 2019
Poster Number:
C-0183
Type:
Educational Exhibit
Keywords:
Cerebrospinal fluid, Diagnostic procedure, MR, Neuroradiology brain
Authors:
A. Hilario Barrio, E. Salvador, P. Martín Medina, L. Koren, G. Ayala, A. Martinez de Aragon, J. M. Millan, F. Ballenilla, A. Ramos Gonzalez; Madrid/ES
DOI:
10.26044/ecr2019/C-0183

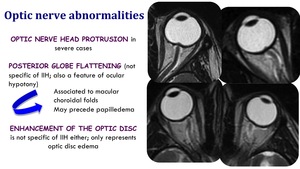
Fig. 10:
Optic nerve abnormalities in IIH

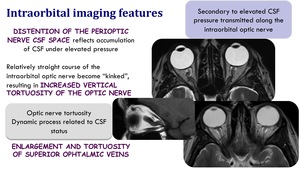
Fig. 11:
Intraorbital imaging features in IIH

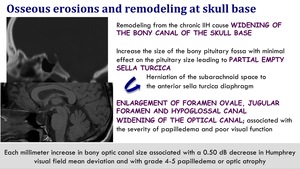
Fig. 12:
Osseous erosions and remodelling at skull base in IIH

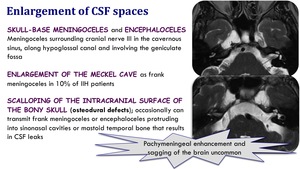
Fig. 13:
Enlargement of CSF spaces in IIH

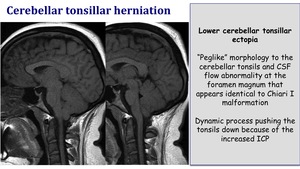
Fig. 14:
Cerebellar tonsillar herniation in IIH

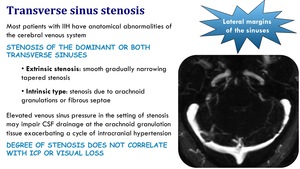
Fig. 15:
Transverse sinus stenosis in IIH

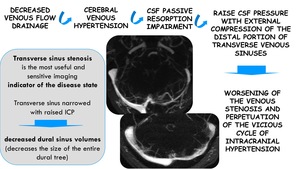
Fig. 16:
Physiopathology of IIH and transverse sinus stenosis

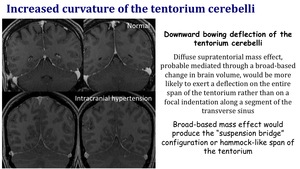
Fig. 17:
Increased curvature of the tentorium cerebelli in IIH

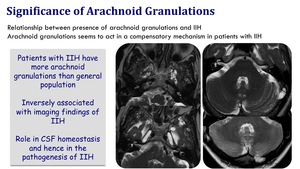
Fig. 18:
Significance of arachnoid granulations in IIH

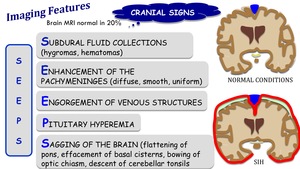
Fig. 19:
Imaging features of spontaneous intracranial hypotension

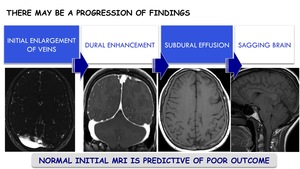
Fig. 20:
Progression of brain MRI findings in SIH

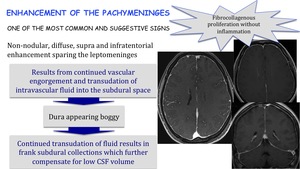
Fig. 21:
Enhancement of the pachymeninges in SIH

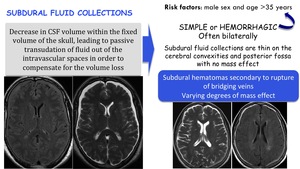
Fig. 22:
Subdural fluid collections in SIH

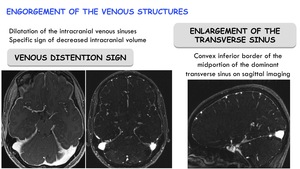
Fig. 23:
Engorgement of the venous structures in SIH

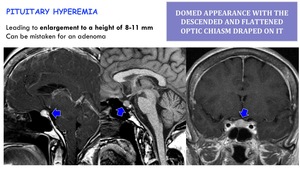
Fig. 24:
Pituitary hypermia in SIH

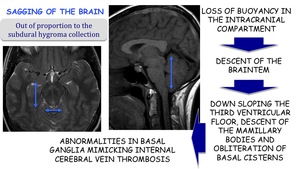
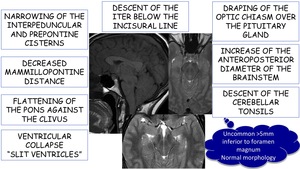
Fig. 25:
Sagging of the brain in SIH

Fig. 26:
Other imaging findings related to sagging brain in SIH

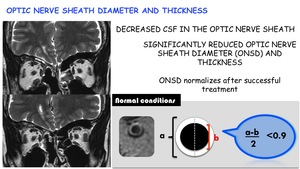
Fig. 27:
Optic nerve sheath diameter and thickness in SIH

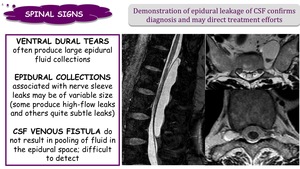
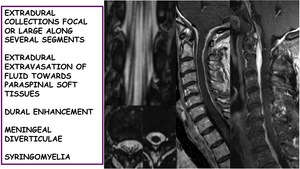
Fig. 28:
Spinal signs in SIH

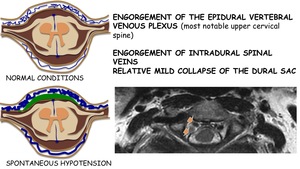
Fig. 29:
Spinal venous engorgement in SIH

Fig. 30:
Other spinal findings in SIH

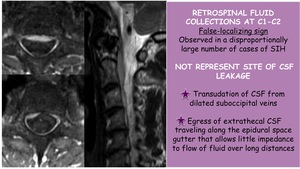
Fig. 31:
Retrospinal fluid collections at C1-C2 in SIH