ECR 2019 / C-0369
Acute Ischemic Stroke: how to make a brilliant report
Congress:
ECR 2019
Poster Number:
C-0369
Type:
Educational Exhibit
Keywords:
Neuroradiology brain, Emergency, CT, CT-Angiography, Diagnostic procedure, Ischaemia / Infarction
Authors:
I. NAVAS FERNANDEZ-SILGADO1, L. Ibañez Sanz1, F. Ballenilla1, P. A. Encinas Escobar2, G. GARCIA GALARRAGA1, J. García Prieto1, J. Alonso Sánchez1, M. D. C. CRUZ CONDE1; 1Madrid/ES, 2Madrid /ES
DOI:
10.26044/ecr2019/C-0369
.
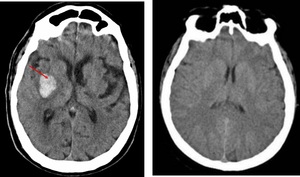
Ischemic stroke (1h of onset of PACI symptoms). Normal CT.")
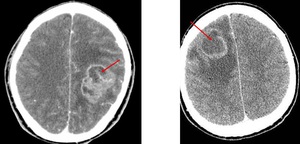
Fig. 4:
Non-contrast CT. Hemorrhage stroke (hypertensive basal ganglia bleed).
...

Fig. 5:
Contrast-enhancement CT. Left frontoparietal glioblastoma multiforme....
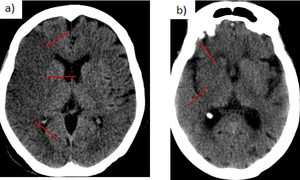
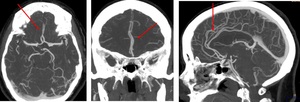
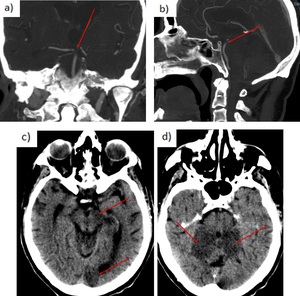
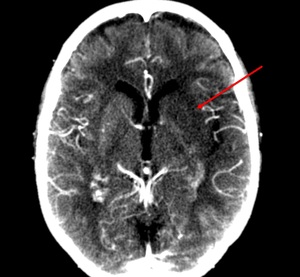
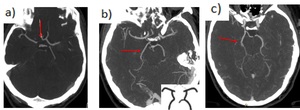
 Loss of gray white mater differentiation with diffuse hypoattenuation involving right MCA territory. Cortical sulcal effacement. b) Obscuration of right caudate and lentiform nucleus. Insular ribbon sign.")
Fig. 6:
a) Loss of gray white mater differentiation with diffuse hypoattenuation...
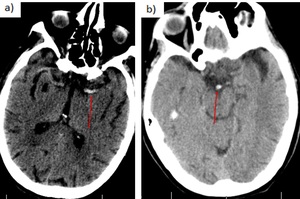
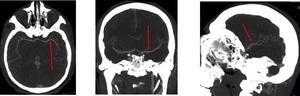
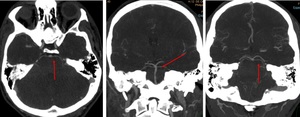
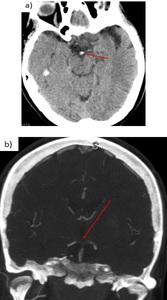
 Dense MCA sign (segment M1 of left MCA). b) Dense basilar sign.")
Fig. 7:
Hyperdensity of a large vessel: a) Dense MCA sign (segment M1 of left MCA). b)...
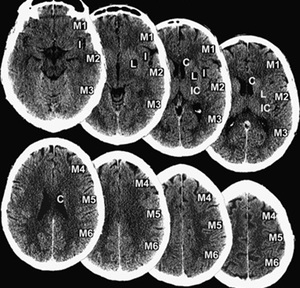
, L (lentiform nucleus), and IC (internal capsule); MCA cortex is allotted 7 points: insular cortex, M1, M2, M3, M4, M5 and M6) . References: Al-Ajlan et al.(2017). Multimodality CT based imaging to determine clot characteristics and recanalization with intravenous tPA in patients with acute ischemic stroke. Neurovascular Imaging")
Fig. 8:
ASPECTS. 1 point is deducted from the initial score of 10 for every region...

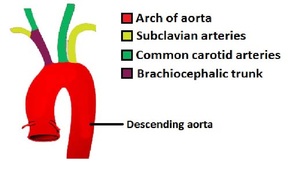
Fig. 9:
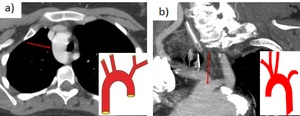
Schematic of the Aortic arch and major branches.
. Radiopaedia, 2009.")
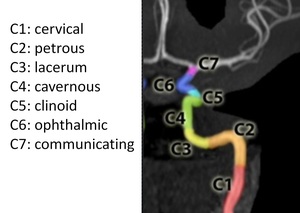
Fig. 10:
Internal carotid artery. Segments.
. Evaluación vascular en el código ictus: papel de la angio-tomografía computarizada. Radiología.")
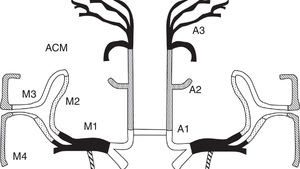
Fig. 11:
Segments of MCA and ACA
. Axial, coronal, sagittal.")
Fig. 12:
Medial cerebral artery (MCA). Axial, coronal, sagittal.
. Axial, coronal, sagittal.")
Fig. 13:
Anterior cerebral artery (ACA). Axial, coronal, sagittal.

Fig. 14:
Basilar artery. Axial, coronal, sagittal.
. Axial, coronal, sagittal.")
Fig. 15:
Posterior cerebral artery (PCA). Axial, coronal, sagittal.

Fig. 16:
Superior cerebellar artery. Axial, coronal, sagittal.
. Axial.")
Fig. 17:
Posteroinferior cerebellar artery (PICA). Axial.
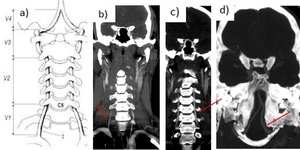
 Segments. V1 (preforaminal, from its origin in the subclavia artery to C6 vertebra). V2 (foraminal, from C6 to C2). V3 (atlantic. C2-C1). V4 (intracranial).
b) V1 segment. c) V2 segment. d) V4 segment.")
Fig. 18:
Vertebral arteries. a) Segments. V1 (preforaminal, from its origin in the...
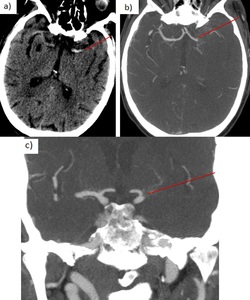
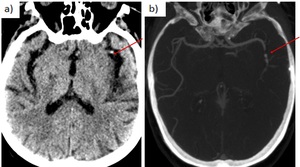
 Non-contrast CT: hyperdense left MCA sign.
b) Axial CTA: occlusion left M1 MCA. Grade 1 leptomeningeal collaterals (<50%). c) Coronal CTA: occlusion left M1 MCA.")
Fig. 19:
78 yo man with right hemiparesis. Ischemic stroke. a) Non-contrast CT:...
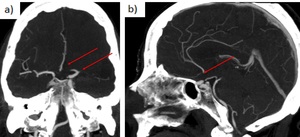
 72 yo man with right hemiparesis. Ischemic stroke. Axial non-contrast CT showing MCA dot sign (left M2 segment in the Sylvian fissure is hyperdense).
b) 79 yo woman with Broca’s aphasia. Axial CTA: short occlusion left M2 MCA.")
Fig. 20:
a) 72 yo man with right hemiparesis. Ischemic stroke. Axial non-contrast CT...
 coronal CTA. B) sagittal CTA.")
Fig. 21:
67 yo woman with right hemiparesis and global aphasia. Occlusion ACA, MCA and...
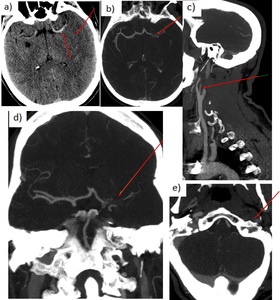
. a) Dense MCA sign (segment M1 of left MCA), diffuse hypoattenuation involving left MCA territory and cortical sulcal effacement. b) Axial CTA: occlusion left M1. c) Sagittal CTA: complete occlusion of the left ICA 2 cm from its origin. d) Coronal CTA: occlusion left M1. e) Axial CTA: lack of contrast enhancement in petrous segment left ICA.")
Fig. 22:
45 yo man with tandem occlusion (left ICA+MCA). a) Dense MCA sign (segment M1...
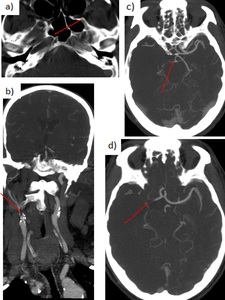
 axial and coronal CTA: complete occlusion right ICA 1 cm from its origin. c-d) axial CTA: occlusion of the right A1 segment, M1 segment, and PCA (fetal origin). Poor collateral flow.")
Fig. 23:
58 yo man with acute left-sided hemiplegia. Right carotid T occlusion. a-b)...
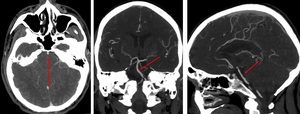
 Coronal and sagittal CTA: filling defect at the top of the basilar artery and in the left P1 segment. Right PCA and both superior cerebellar arteries are well opacified with contrast.
c - d) Non-contrast CT 1 month later: low density (infarction) involving the left midbrain, the inferior portion of the temporal lobe and occipital lobe, and cerebellum.")
Fig. 24:
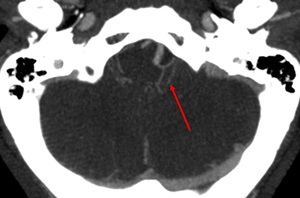
a - b) Coronal and sagittal CTA: filling defect at the top of the basilar...
 The top of the basilar artery is markedly hyperdense. b) CTA confirms the presence of a filling defect at the top of the basilar artery and both P1 segments of the PCA.")
Fig. 25:
66 yo woman. She falls down and enters a coma. a) The top of the basilar artery...
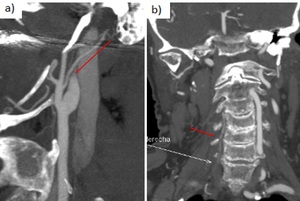
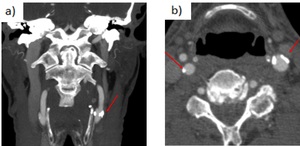
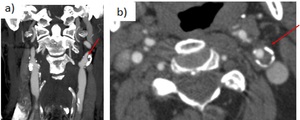
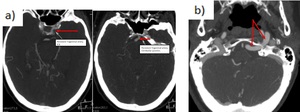
 Dissection of the left cervical ICA in a 48 yo woman. Sagittal CTA shows the typical flame-like shape occlusion 3 cm above the carotid bifurcation.
b) Dissection of the right vertebral artery in a 63 yo man. Coronal CTA shows an irregularity of the right vertebral artery from its origin.")
Fig. 26:
a) Dissection of the left cervical ICA in a 48 yo woman. Sagittal CTA shows the...
. b) Grade 2 (> 50%)")
Fig. 27:
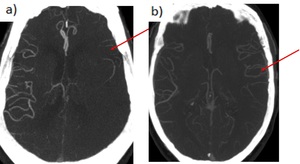
Leptomeningeal collaterals. Grade 1 (< 50%). b) Grade 2 (> 50%)
.")
Fig. 28:
CTASI shows hypoattenuating left MCA territory (caudate and lentiform nucleus,...
. a) Coronal CTA. b) Axial CTA.")
Fig. 29:
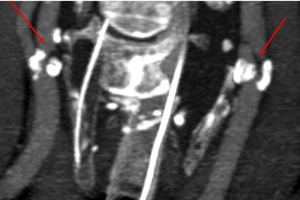
Carotid bulbs calcium plaques with no significant stenosis (<50%). a) Coronal...
. a) Coronal CTA. b) Axial CTA.")
Fig. 30:
Mixed atheromatous plaques with left ICA severe stenosis (>70%). a) Coronal...

Fig. 31:
Near-occlusion left ICA stenosis. Severe right ICA stenosis. Coronal CTA.
 Right aortic arch.
b) Bovine aortic arch, most common variant of the aortic arch = Inominate artery shares a common origin with the left common carotid artery.")
Fig. 32:
a) Right aortic arch.
b) Bovine aortic arch, most common variant of the aortic...
 Absent A1 segment of ACA.
b) Fetal posterior cerebral artery (estimated to occur in 20%, most common unilateral). P1 is absent. The posterior communicating artery supplies the bulk of the blood to the PCA. If bilateral, the basilar artery is significantly smaller than normal.
c) Partial fetal PCA. Posterior communicating artery is larger than P1.")
Fig. 33:
a) Absent A1 segment of ACA.
b) Fetal posterior cerebral artery (estimated to...
 Persistent primitive trigeminal artery. It is one of the persistent carotid-vertebrobasilar anastomoses (it is a junction between cavernous ICA and basilar artery). It is present in 0,1-0,5%. b) Persistent hypoglossal artery. It is a persistent carotid-vertebrobasilar anastomoses, the second in frequency (0,02-0,1%). It arises from the distal cervical ICA (between C1-C3). After passing through an enlarged hypoglossal canal, it joins the basilar artery inferiorly.")
Fig. 34:
a) Persistent primitive trigeminal artery. It is one of the persistent...

Fig. 35:
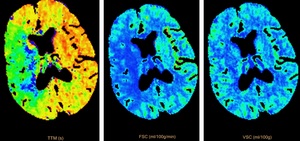
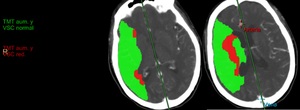
CTP imaging study showing an acute stroke of the right MCA territory with...
.")
Fig. 36:
Same patient. Larger region of right MCA territory penumbra (represented by the...
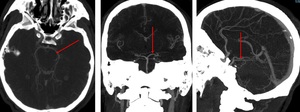
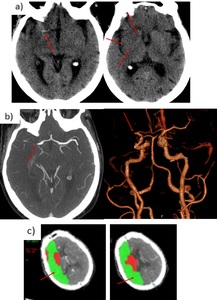
Non-contrast CT. Hyperdense M1 segment of right MCA. Hypoattenuation of the ipsilateral insular cortex and basal ganglia.
b) Axial CTA and 3D reconstruction. Complete occlusion of the right M1 segment just distal to the bifurcation.
c) CTP. Established infarct core in the right MCA territory, with a larger surrounding ischemic penumbra.")
Fig. 37:
72 yo man. Left hemiparesis. Right M1 occlusion.
a)Non-contrast CT. Hyperdense...