ECR 2019 / C-0701
Imaging review of peritoneal anatomy with emphasis on route of spread of pathologies
Congress:
ECR 2019
Poster Number:
C-0701
Type:
Educational Exhibit
Keywords:
Abdomen, Anatomy, Peritoneum, CT, Localisation, Infection, Inflammation, Metastases
Authors:
M. Mohandas, S. Nadarajan, N. Hubert, L. Jose; Thiruvananthapuram/IN
DOI:
10.26044/ecr2019/C-0701
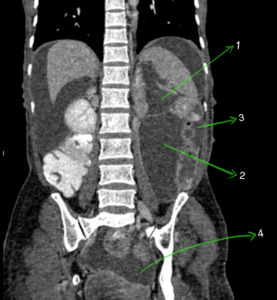
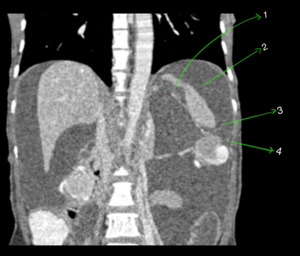
 and adnexal lesions (3) in a patient with neurofibromatosis. A small cutaneous neurofibroma is seen in abdominal wall (1).")
Fig. 4:
Coronal CECT abdomen showing gross ascitis (2) and adnexal lesions (3) in a...
 separating right subphrenic space (3) and left subphrenic space (4). Right triangular ligament (2) is also seen separating right subphrenic space (3) and right sub hepatic space (5).")
Fig. 5:
Axial CECT abdomen showing peritoneal ligaments of liver - falciform ligament ...
 and Hepatoduodenal (2) ligaments.")
Fig. 6:
Axial CECT abdomen showing the two components of lesser omentum - Gastrohepatic...
.")
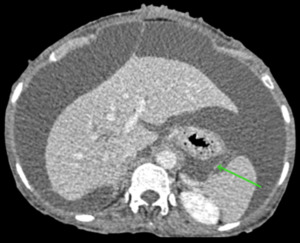
Fig. 7:
Axial CECT abdomen showing the gastrosplenic ligament (green arrow).
.")
Fig. 8:
Sagittal CECT abdomen showing gastrocolic ligament (green arrow).
.")
Fig. 9:
Axial CECT abdomen showing splenorenal ligament (green arrow).
 dividing peritoneal cavity into supramesocolic (2) and inframesocolic spaces (3).")
Fig. 10:
Sagittal CECT abdomen showing transverse mesocolon (1) dividing peritoneal...
.")
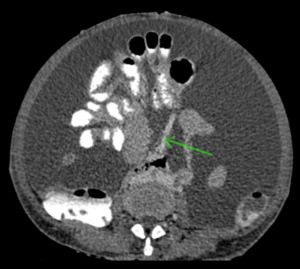
Fig. 11:
Axial CECT abdomen showing small bowel mesentery (green arrow).
.")
Fig. 12:
Coronal CECT abdomen showing sigmoid mesocolon (green arrow).
, inframesocolic space (2), paracolic (3) and pelvic spaces (4).")
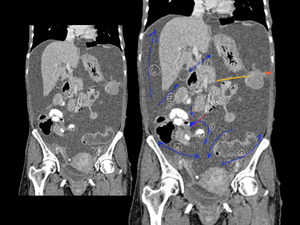
Fig. 13:
Coronal CECT abdomen showing various peritoneal spaces - Supramesocolic space...
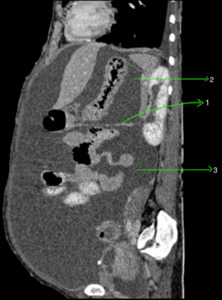
 and perisplenic space (1). Left subphrenic space (2) is separated from left paracolic space (4) by the phrenicocolic ligament (3).")
Fig. 14:
Coronal CECT abdomen showing left supramesocolic space- Left subphrenic space...
 and inferior recess (3) being separated by the peritoneal fold containing left gastric artery (2).")
Fig. 15:
Coronal CECT abdomen showing the two recesses of lesser sac, the superior...
 which is the route of communication between right subhepatic space (1) and inferior recess of lesser sac (2).")
Fig. 16:
Axial CECT abdomen showing Foramen of Winslow (curved red line) which is the...
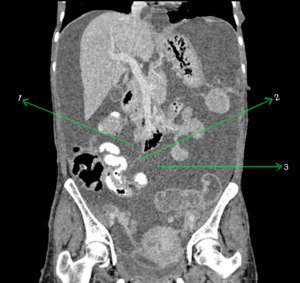
 being limited inferiorly by the attachment of root of mesentery (2) to caecum and the larger left inframesocolic space (3) communicating freely with the pelvis.")
Fig. 17:
Coronal CECT abdomen showing the inframesocolic spaces. The smaller right...
 in the lateral aspect of ascending colon and left paracolic space (2) in the lateral aspect of descending colon.")
Fig. 18:
Coronal CECT abdomen showing the right paracolic space (1) in the lateral...
 and vesicouterine pouch (2).")
Fig. 19:
Sagittal CECT abdomen showing the rectouterine pouch (1) and vesicouterine...

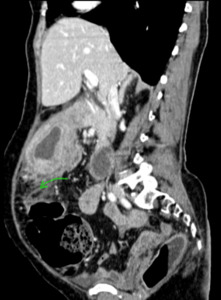
Fig. 20:
Schematic representation of route of spread
.")
Fig. 21:
Sagittal CECT abdomen of a 60 year old female showing spread of gastric...
 infiltrating into mesentery with invasion of superior mesenteric vein (blue arrow). Red arrow is superior mesenteric artery.")
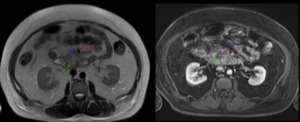
Fig. 22:
Axial MR abdomen of a 52 year old male, T2Wi and post contrast T1Wi showing...
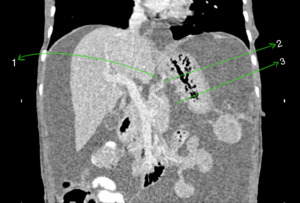
 with a walled off necrosis (P) in head and body. Cranial section of same patient shows fluid collection and inflammation extending to gastrosplenic ligament (asterix).")
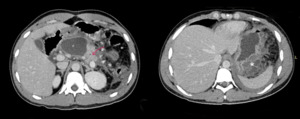
Fig. 23:
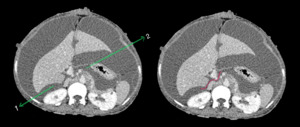
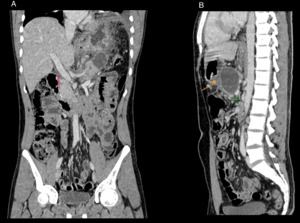
Middle aged male with acute on chronic pancreatitis. CECT abdomen axial...
 and sagittal (B) images of the same patient. In A, red arrow shows rim of hypodensity surrounding portal vein suggestive of spread of inflammation along hepatoduodenal ligament. In B, yellow and green arrows indicate inflammation extending to lesser sac and transverse mesocolon respectively.")
Fig. 24:
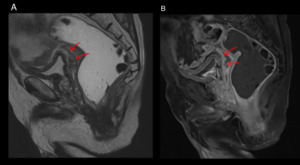
Coronal (A) and sagittal (B) images of the same patient. In A, red arrow shows...
 and post contrast T1 Wi (B) images show necrotic deposit in rectovesical pouch (red arrows), which is the most dependent peritoneal space in men.")
Fig. 25:
Elderly male who is a known case of carcinoma head of pancreas. Sagittal T2 Wi...