ECR 2019 / C-0716
Greater trochanteric pain syndrome: clinical and radiological semiology
Congress:
ECR 2019
Poster Number:
C-0716
Type:
Educational Exhibit
Keywords:
Inflammation, Comparative studies, Ultrasound, MR, Musculoskeletal system, Musculoskeletal soft tissue
Authors:
A. Solano1, A. Agustí2, I. García Duitama2, M. tey3, A. Rodriguez Baeza3, J. Ares Vidal2; 1BARCELONA, BARCELONA/ES, 2Barcelona/ES, 3Barcelona /ES
DOI:
10.26044/ecr2019/C-0716

Fig. 8:
Criteria for diagnosis of Greater Trochanteric Pain Syndrome

Fig. 9:
Clinical Test

Fig. 10:
Clinical Test

Fig. 11:
Clinical Test

Fig. 12:
Plain radiography.

Fig. 13:
Plain radiography.

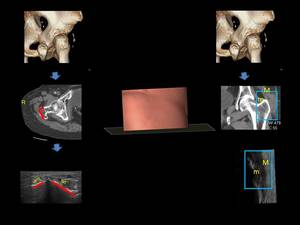
Fig. 14:
Radiological Correlation.
")
Fig. 15:
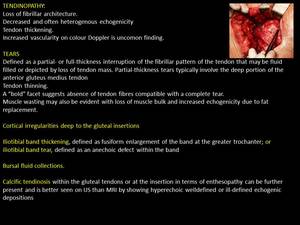
Morphological findings (text)
")
Fig. 16:
Morphological findings (images)

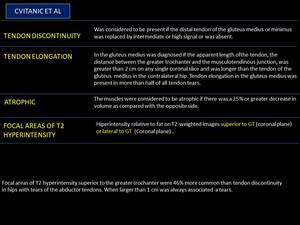
Fig. 17:
Cvitanic et al

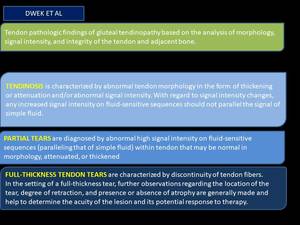
Fig. 18:
Dwek et al

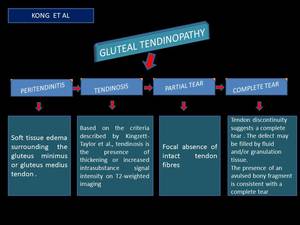
Fig. 19:
Kong et al

Fig. 20:
Normal MRI anatomy

Fig. 21:
Pathological MRI findings

Fig. 22:
Pathological MRI findings

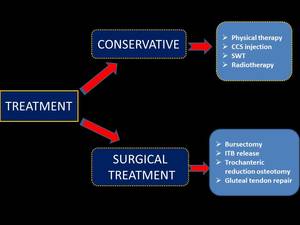
Fig. 23:
Management of the greater trochanteric pain syndrome

Fig. 24:
Hip Arthroscopy