ECR 2019 / C-0774

Diagnostic accuracy of TIRADS in evaluation of thyroid nodules
Congress:
ECR 2019
Poster Number:
C-0774
Type:
Scientific Exhibit
Keywords:
Head and neck, Thyroid / Parathyroids, Ultrasound, Diagnostic procedure, Calcifications / Calculi, Cysts, Neoplasia
Authors:
M. Mohandas, S. Nadarajan, N. Hubert, L. Jose; Thiruvananthapuram/IN
DOI:
10.26044/ecr2019/C-0774

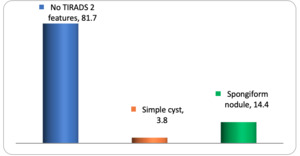
Fig. 8:
Percentage distribution of sample according to TIRADS 2 features

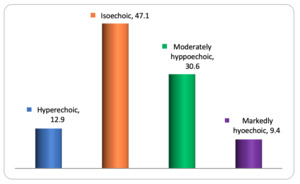
Fig. 9:
Percentage distribution of sample according to echogenicity in TIRADS 3, 4 & 5...

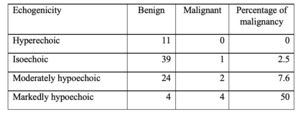
Table 1:
Distribution of sample according to echogenicity and percentage of malignancy...

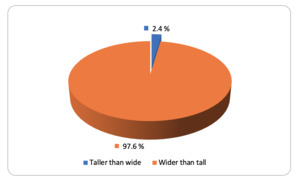
Fig. 10:
Percentage distribution of sample according to shape in TIRADS 3, 4 & 5 nodules

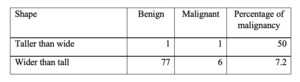
Table 2:
Distribution of sample according to shape and percentage of malignancy in...

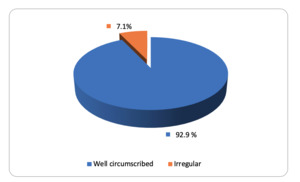
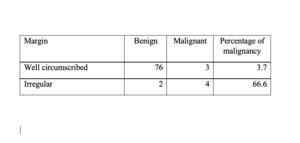
Fig. 11:
Percentage distribution of sample according to margin in TIRADS 3, 4 & 5 nodules

Table 3:
Distribution of sample according to margin and percentage of malignancy in...

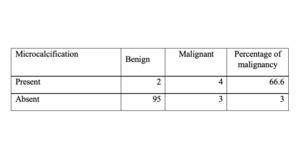
Fig. 12:
Percentage distribution of sample according to microcalcification

Table 4:
Distribution of sample according to microcalcification and percentage of...

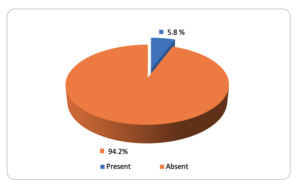
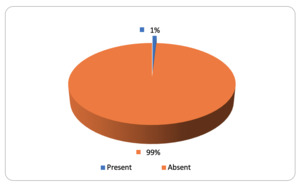
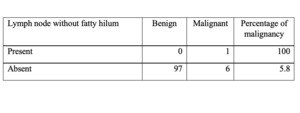
Fig. 13:
Percentage distribution of sample according to lymph node without fatty hilum

Table 5:
Distribution of sample according to presence of lymph nodes without fatty hilum...

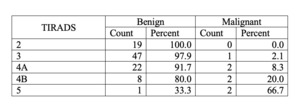
Table 6:
Association of TIRADS with cyto/histopathological result

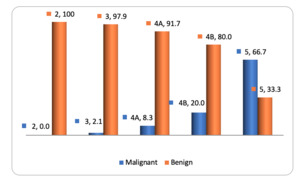
Fig. 14:
Bar diagram showing ssociation of TIRADS with cyto/histopathological result

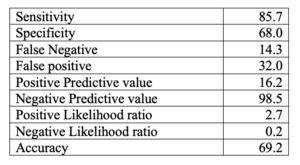
Table 7:
Statistical indices showing comparison of TIRADS with histopathology.

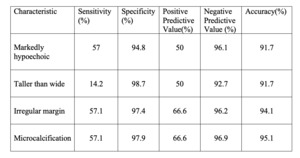
Table 8:
Diagnostic test properties of sonological findings of malignant nodules
 References: Dr. Minu Mohandas")
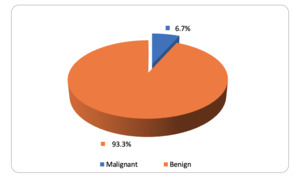
Fig. 15:
Percentage distribution of sample according to cyto/ histopathology (benign/...

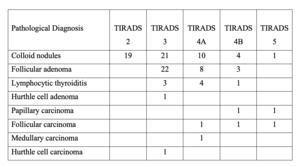
Table 9:
Retrospective comparison of pathological diagnosis with assigned TIRADS...

Fig. 16:
Transverse sonogram of thyroid gland showing spongiform nodule with echogenic...

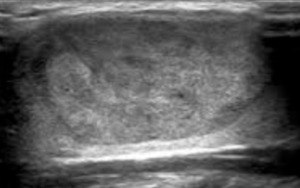
Fig. 17:
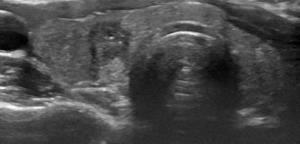
Transverse thyroid sonogram showing a predominantly solid wider than tall...

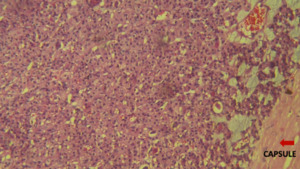
Fig. 18:
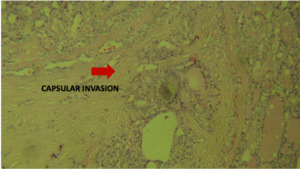
Photomicrograph demonstrating histologic features of follicular adenoma with...

Fig. 19:
Transverse thyroid sonogram showing a wider than tall isoechoic nodule with...
. References: Department of Pathology, Dr. Somervell Memorial CSI Medical College, Thiruvananthapuram/IN")
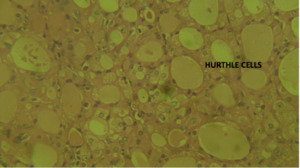
Fig. 20:
Photomicrograph demonstrating histologic features of Hurthle cell carcinoma...

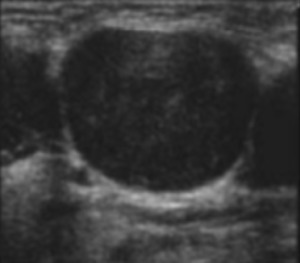
Fig. 21:
Transverse sonogram of thyroid showing a taller than wide markedly hypoechoic...

Fig. 22:
Photomicrograph demonstrating histologic features of follicular carcinoma with...

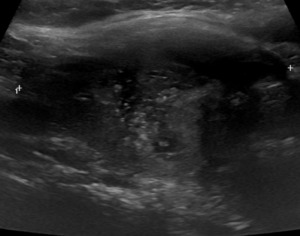
Fig. 23:
Transverse sonogram of thyroid showing a markedly hypoechoic nodule with...

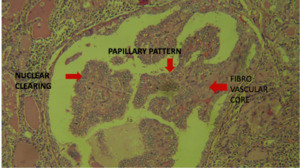
Fig. 24:
Photomicrograph demonstrating histologic features of papillary carcinoma with...

Fig. 25:
Transverse sonogram of thyroid showing a moderately hypoechoic nodule in the...

Fig. 26:
Photomicrograph demonstrating histologic features of Medullary carcinoma with...

Fig. 27:
Transverse neck sonogram of patient shows a cervical lymph node which had round...

Fig. 28:
Transverse sonogram of thyroid gland showing a taller than wide markedly...