ECR 2019 / C-0913

Hydatid disease from Head to Toe - A pictorial review
Congress:
ECR 2019
Poster Number:
C-0913
Type:
Educational Exhibit
Keywords:
Abdomen, Head and neck, CT, MR, Ultrasound, Diagnostic procedure, Infection
Authors:
G. Ilangovan, M. Saravanan; Chennai, TA/IN
DOI:
10.26044/ecr2019/C-0913
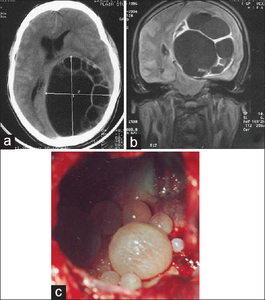
 Plain computed tomography scan of brain, axial view: Showing a large multi-cystic lesion in left parieto-occipital region with mass effect.
(b) Plain magnetic resonance imaging scan of brain T1, coronal view: Showing a large multi-cystic lesion in left parieto-occipital region with mass effect.
(c) Intraoperative findings confirm multiple daughter cysts inside a large cyst References: Senapati SB, Parida DK, Pattajoshi AS, Gouda AK, Patnaik A. Primary hydatid cyst of brain: Two cases report. Asian journal of neurosurgery. 2015 Apr;10(2):175.")
Fig. 3:
(a) Plain computed tomography scan of brain, axial view: Showing a large...
:643-7.")
Fig. 5:
Thyroid ultrasonography showed two neighboring nodular, hypoheterogenous...
:475-94.")
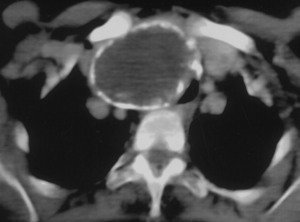
Fig. 4:
Axial CT scan through the upper mediastinum shows a hypoattenuating mass with...
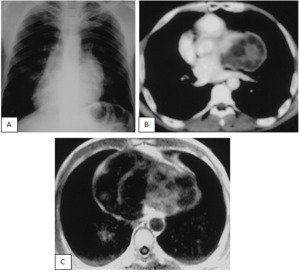
 Chest radiograph shows multiple hydatid cysts located in both lungs as well-defined lesions.
(b) CT scan shows multiple hydatid cysts in both lungs as well-demarcated cystic masses. References: Emlik D, Ödev K, Poyraz N, Kaya HE. Radiological Characteristics of Pulmonary Hydatid Cysts. InCurrent Topics in Echinococcosis 2015. InTech.")
Fig. 6:
(a) Chest radiograph shows multiple hydatid cysts located in both lungs as...
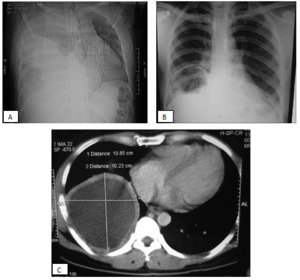
 Chest X-ray on admission showed a homogenous right sided opacity
(massive pleural effusion) with mediastinal shift
(B) Chest X-ray after pleural fluid drainage showed a cystic structure in right lung base
(C) Thick, smooth walled contrast-enhanced pleural based cystic structure on contrast enhanced computed tomography thorax suggestive of pleural based hydatid cyst
References: Chakrabarti S, Patra A, Biswas P, Mandal K. Pulmonary hydatid cyst presenting as massive unilateral pleural effusion. The Journal of Association of Chest Physicians. 2015 Jan 1;3(1):20.")
Fig. 7:
(A) Chest X-ray on admission showed a homogenous right sided opacity
...
:475-94.")
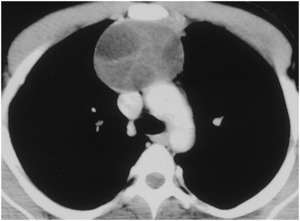
Fig. 8:
Anterior mediastinal type IIB HC. Axial contrast-enhanced CT scan shows an HC...
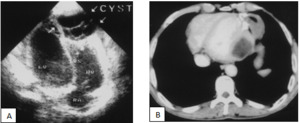
 HD of the heart in a 28-year-old woman. Transverse US image shows a multiloculated anechoic mass with daughter cysts in the right ventricle (arrows), a finding that is consistent with type IIB HC. IVN = interventricular septum, LV = left ventricle, RA = right atrium, RV = right ventricle.
(B) HD of the heart in a 43-year-old man. Axial contrast-enhanced CT scan shows a low-attenuation mass in the left ventricle, a finding that is consistent with type I unilocular HC.
References: Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. Radiographics. 2003 Mar;23(2):475-94.")
Fig. 9:
(A) HD of the heart in a 28-year-old woman. Transverse US image shows a...
 Posteroanterior chest radiograph shows deformation of the lung contour at the left border of the heart, which is obscured by a radiopaque lesion. Note also the displacement of the heart to the right.
(B) Axial contrast-enhanced CT scan shows a type IIA HC with multiple peripheral daughter cysts.
(C) Axial spin-echo T1-weighted MR image also shows a type IIA HC in proximity to the left ventricular wall and displacing the heart to the right.
References: Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. Radiographics. 2003 Mar;23(2):475-94.")
Fig. 10:
HD with pericardial involvement in a 15-year-old boy.
(A) Posteroanterior...
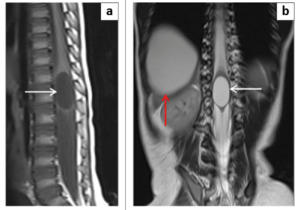
 and coronal T2-weighted (b) images demonstrate an intamedullary cystic lesion (white arrows) that follows CSF signal intensity on all sequences and did not show post-contrast enhancement. Associated finding of a hepatic hydatid cyst (red arrow). References: Bezuidenhout AF, Lipsitz JM, Du Plessis AM. Intramedullary spinal masses: A pictorial essay. SA Journal of Radiology. 2014 Oct;18(1):1-7.")
Fig. 11:
Rare case of an intramedullary conus medullaris echinococcus cyst in a...
 indicating degeneration of the germinal layer. References: Czermak BV, Akhan O, Hiemetzberger R, Zelger B, Vogel W, Jaschke W, Rieger M, Kim SY, Lim JH. Echinococcosis of the liver. Abdominal imaging. 2008 Mar 1;33(2):133-43.")
Fig. 12:
A 65-year-old woman with liver hydatid cyst in degeneration. Enhanced CT scan...
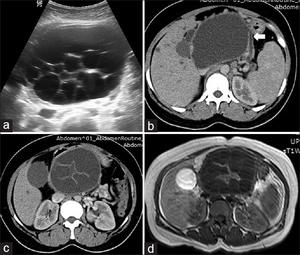
 Ultrasound abdomen shows multiloculated cystic lesion. (b) Postcontrast axial computed tomography scan shows cystic lesion in the pancreatic head having communication with dilated main pancreatic duct (arrow in b) with the curvilinear internal membrane. (c) T1-.weighted axial magnetic resonance imaging image. (d) Internal daughter cysts having hyperintense cyst wall and central hyperintense floating membrane References: Choudhary P, Khokhar HV, Aswani Y, Saxena S. Preoperatively diagnosed isolated hydatid cyst of pancreatic head with triad of obstructive jaundice, left-sided portal hypertension and chronic pancreatitis. MAMC Journal of Medical Sciences. 2015 Sep 1;1(3):157.")
Fig. 13:
(a) Ultrasound abdomen shows multiloculated cystic lesion. (b) Postcontrast...
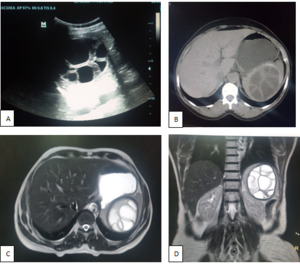
 USG b-mode image shows a well-defined cystic lesion with multiple septations and posterior acoustic enhancement within the spleen, suggestive of spleenic Hydatid cyst with daughter cysts within.
(B) On CT, A well-defined hypodense lesion with a hydatid matrix and peripheral daughter cysts is noted in the upper part of the spleen.Splenic cyst with internal septations give the appearance of daughter cysts, in keeping with hydatid cyst.
On MRI (C) Axial and (D) Coronal T2WI shows a hyper intense, multicystic lesion with multiple daughter cysts.
References: Department of radiology, shri sathya sai medical college and research institute, Tamilnadu/ India 2018")
Fig. 17:
(A) USG b-mode image shows a well-defined cystic lesion with multiple...
 Coronal section of contrast-enhanced computed tomography scan revealing a large well-defined expansile soft tissue hypo-attenuating mass lesion showing multiple cystic areas within it suggestive of hydatid, arising from cortex of upper pole of left kidney. (b) Axial section of contrast-enhanced computed tomography scan showing the large multiseptate left renal hydatid cyst. This image is typical of Type 2 cysts, which are multilocular with mixed internal attenuation, contain multiseptated daughter cysts References: Gupta M, Singh R, Lehl SS. Isolated renal hydatid cyst in a diabetic postmenopausal female. Journal of mid-life health. 2015 Jul;6(3):134.")
Fig. 14:
(a) Coronal section of contrast-enhanced computed tomography scan revealing a...
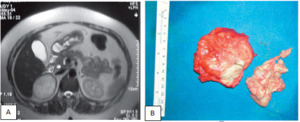
 An MRI scan of the abdomen demonstrated a 4.5 x 3.5 x 3 cm homogenous solid adrenal mass on the right side. Moderate hyperintensity in T2WI is present and peripheral rim-like contrast enhancement was obtained after contrast administration. No other intra-abdominal masses were found.
(B) In the cross sections of the specimen after removal, daughter cysts and the existence of a germinating membrane revealed a hydatid cyst. Histopathologic examination confirmed hydatid disease in the adrenal gland.
References: Özarmagan S, Erbil Y, Barbaros U, Salmaslioglu A, Bozbora A. Primary hydatid disease in the adrenal gland: a case report. Brazilian Journal of Infectious Diseases. 2006 Oct;10(5):362-3.")
Fig. 15:
(A) An MRI scan of the abdomen demonstrated a 4.5 x 3.5 x 3 cm homogenous solid...
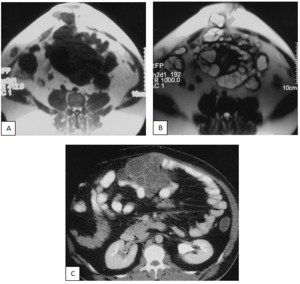
 Axial breath-hold fast spin-echo T1-weighted MR image shows multiple low-signal-intensity lesions within the mesenteric fatty tissue. Note also the umbilical hernia and the low-signal-intensity masses within the herniated sac.
(B) Corresponding axial rapid acquisition with relaxation enhancement T2-weighted MR image shows multiple areas of increased signal intensity. The hypointense rim sign characteristic of HCs is best seen with this sequence. Note also the multivesicular hepatic cyst within the herniated sac.
(C) Peritoneal HD in a 47-year-old man who had previously undergone surgery for a hepatic HC. Axial contrast-enhanced CT scan through the middle pole of the kidneys shows multiple low-attenuation daughter cysts in the peritoneal cavity.
References: Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. Radiographics. 2003 Mar;23(2):475-94.")
Fig. 16:
Intraperitoneal HCs and a herniated umbilical sac in a 55-year-old man with a...
 Axial contiguous
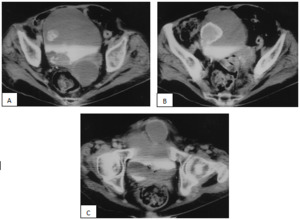
contrast-enhanced CT scan through the lower pelvis shows low-attenuation masses in the left retrovesical area.
The posterolateral bladder wall is seen to protrude into the lumen of the bladder. Note the intralesional calcification, which originates at the right posterolateral wall. In addition, there is a second, densely calcified lesion
within the bladder lumen (type III hepatic cyst). (B) Axial contrast-enhanced CT scan obtained 10 mm distal
to a shows a hypoattenuating mass with dense peripheral calcification that protrudes into the bladder lumen.
(C) Axial contrast-enhanced CT scan obtained 10 mm distal to b shows a third low-attenuation mass that protrudes from the anterior wall of the bladder. References: Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. Radiographics. 2003 Mar;23(2):475-94.")
Fig. 18:
Secondary involvement of the bladder and retrovesical areas in a 53-year-old...
:475-94.")
Fig. 19:
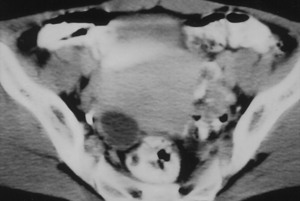
Incidentally found HD with primary ovarian involvement in a 38-year-old woman....
:475-94.")
Fig. 20:
HD with secondary scrotal involvement in a 63-year-old man with multiple HCs in...
:475-94.")
Fig. 21:
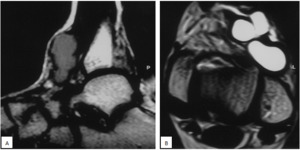
Primary type I HC of the psoas muscle in a 46-year-old woman who presented with...
 Sagittal proton-density–weighted MR image shows a low-signal-intensity mass with a hypointense rim at the dorsal surface of the left ankle. (B) Axial T2-weighted MR image shows multiple homogeneous masses with increased signal intensity. Note also the hypointense rim at the periphery of the lesions. References: Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. Radiographics. 2003 Mar;23(2):475-94.")
Fig. 22:
Soft-tissue HD in a 27-year-old man who presented with palpable masses at the...
:475-94.")
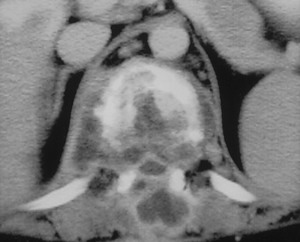
Fig. 23:
Vertebral HD with secondary spinal canal involvement in a 45-year-old woman who...