ECR 2019 / C-1001
Interventional radiology in multiple myeloma
Congress:
ECR 2019
Poster Number:
C-1001
Type:
Educational Exhibit
Keywords:
Education and training, Vertebroplasty, Diagnostic procedure, CT, Interventional non-vascular
Authors:
S. Carbullanca Toledo, I. García Duitama, A. Agustí, A. Solano, J. Ares, C. V. Martinez Stocker, M. Vilas Gonzalez; Barcelona/ES
DOI:
10.26044/ecr2019/C-1001

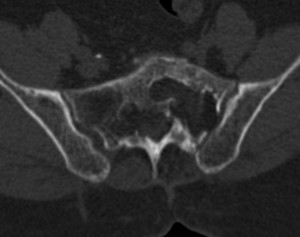
Fig. 1

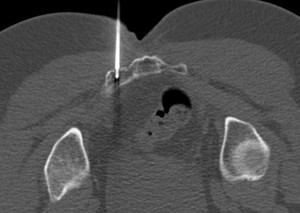
Fig. 2:
CT guided iliac biopsy

Fig. 3:
70 years. Low back pain
History of plasmacytoma treated with RT.

Fig. 4:
Result: Post-treatment changes

Fig. 5:
Normal bone

Fig. 6:
40 years

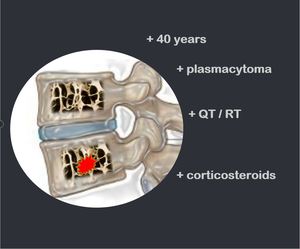
Fig. 7:
40 years / plasmacytoma / QT/RT / corticosteroids

Fig. 8:
Flat vertebra

Fig. 9:
Canal / Foraminal severe stenosis

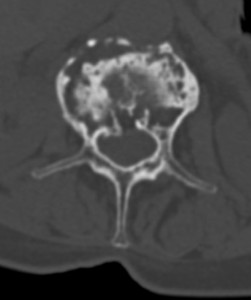
Fig. 10:
Image compatible with vertebral fracture +/- focal lesion

Fig. 11:
Image compatible with vertebral fracture +/- focal lesion

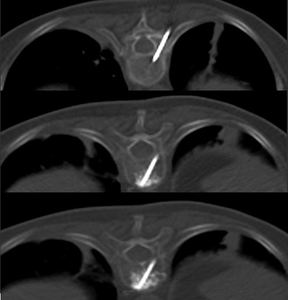
Fig. 12:
Injection of bone cement into the fractured bodies.

Fig. 13:
Injection of bone cement into the fractured bodies.

Fig. 14:
Injection of bone cement into the fractured bodies.

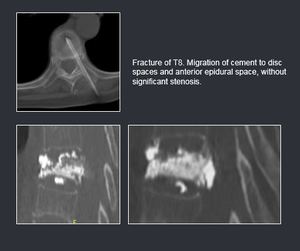
Fig. 16:
Complications

Fig. 15:
Injection of bone cement into the fractured bodies.