Type:
Educational Exhibit
Keywords:
Acute, Catheters, MR, CT, Catheter arteriography, Neuroradiology brain, Interventional vascular, Haemorrhage
Authors:
G. Monedero Herrador1, M. Martínez-Galdámez1, J. Escartín López2, C. Rodriguez Fernandez1, A. Hermosin Pena1, J. Periáñez1; 1Madrid/ES, 2Majadahonda, Madrid/ES
DOI:
10.26044/ecr2019/C-1004
Background
CAUSES OF SAH
Although trauma is the most common cause of SAH,
ruptured saccular aneurysms are the most common cause of nontraumatic SAH,
accounting for approximately 85% of cases of spontaneous SAH.
Of the remaining 15% of cases,
two thirds are due to idiopathic perimesencephalic hemorrhage,
a benign non-aneurysmal form of SAH that is likely venous in origin.
The remaining cases result from a wide variety of causes.
[1]
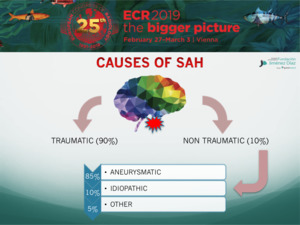
Fig. 2
PATTERNS OF BLOOD DISTRIBUTION
SAH can be classified into at least three distinct patterns by location on initial unenhanced CT.
Recognizing these patterns facilitates the differential diagnosis and refines further imaging evaluation.
Proper classification depends on unenhanced CT evaluation within 3 days of symptom onset,
because substantial redistribution occurs thereafter,
fundamentally altering the pattern [1]:
- In the first pattern,
SAH is centered in the suprasellar or central basal cisterns and extends peripherally in a diffuse manner.
This pattern is characteristic of saccular aneurysm rupture but may occur with other entities,
such as rupture of a non-saccular aneurysm or vascular malformation.
- In the second pattern,
SAH is centered in the perimesencephalic or low basal cisterns and does not extend peripherally.
This pattern is characteristic of idiopathic perimesencephalic hemorrhage but results from vertebrobasilar aneurysm rupture in approximately 5% of cases.
Other rare causes of the perimesencephalic pattern include a cervicomedullary junction tumor,
vascular malformation,
or acute arterial dissection.
- In the third pattern,
SAH is localized to the cerebral convexities alone.
This pattern is infrequent,
and the differential diagnosis encompasses a heterogeneous group of diseases.
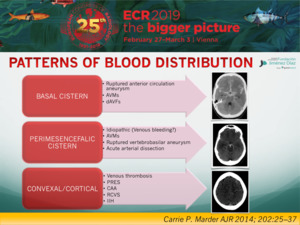
Fig. 3
CORTICAL SAH: ETIOLOGY
Spontaneous acute cSAH observed at the convexity of the brain is a relatively rare entity,
seldom described, with various vascular and nonvascular causes,
including the following: CVT (both dural and cortical),vascular malformations (pial arteriovenous malformations,
dural arteriovenous fistulas,
and cavernomas),
RCVS,vasculitides, infectious aneurysms,Moyamoya disease or syndrome,severe atherosclerotic carotid disease,
PRES, CAA, and nonvascular disorders,
such as primary and secondary brain neoplasmsor even abscess.
[2]
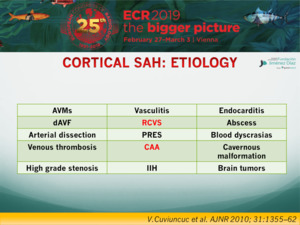
Fig. 4
CORTICAL SAH: CLINICAL PRESENTATION
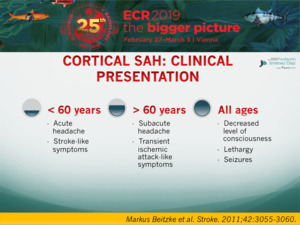
Fig. 5
The purposes of this work were the following: first to propose a diagnostic work-up that covers the wide spectrum of potential underlying causes of cSAH and then to review the specific findings of some etiology that may be responsible for cSAH.
PROTOCOL
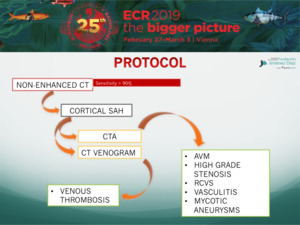
Fig. 6
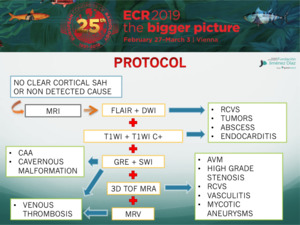
Fig. 7
