ECR 2019 / C-1420
Mulling over Mullerian duct anomalies
Congress:
ECR 2019
Poster Number:
C-1420
Type:
Educational Exhibit
Keywords:
Education and training, Education, MR, Pelvis
Authors:
R. S1, S. GOPALAN2, A. Nagadi3, M. Kapanigowda1, M. Kumar3, N. Perothayil1, R. Jadiya4, F. SHAFI1, S. R. Khan3; 1BENGALURU/IN, 2BANGALORE, KARNATAKA/IN, 3Bangalore/IN, 4bangalore, ka/IN
DOI:
10.26044/ecr2019/C-1420
")
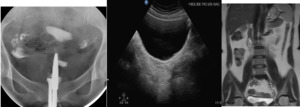
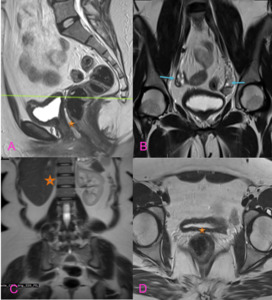
Fig. 2:
Images of HSG demonstrating normal uterine contour, USG pelvis and coronal MRI...
 and coronal MRI images (C, D) showing complete duplication of uterine horns (blue arrow indicating the right uterine horn and red arrow indicating the left uterine horn). Features are suggestive of Uterine Didelphis (Bicornis Bicollis).")
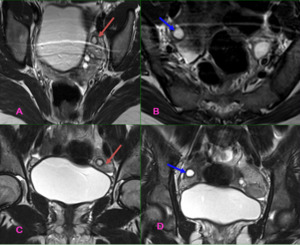
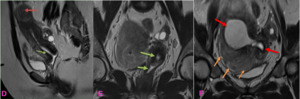
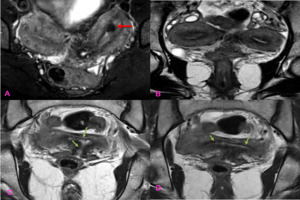
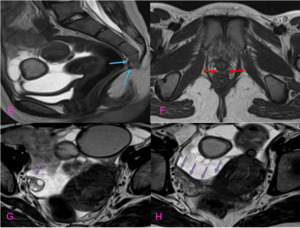
Fig. 3:
T2 axial (A, B) and coronal MRI images (C, D) showing complete duplication of...
 showing complete duplication of uterine horns and cervices with widely separated horns located along the supero-lateral aspect of urinary bladder (blue arrow indicating the right and red arrow indicating the Left).
T1 FS MRI images (E) demonstrates hyperintense fluid seen in right uterine horn (blue arrow) suggestive of Hematometra.
T2 sagittal MRI (F) image of mid pelvis, showing absent uterus in the midline.")
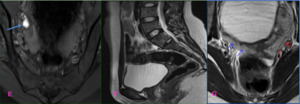
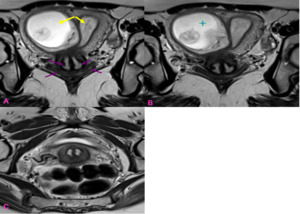
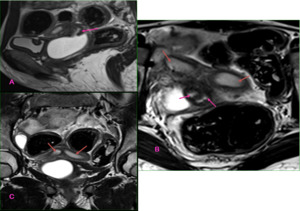
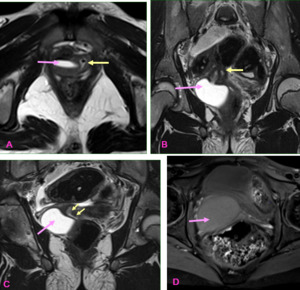
Fig. 4:
T2 axial MRI image (G) showing complete duplication of uterine horns and...
 and coronal images MRI images (A,C) demonstrating Bicornuate unicollis uterus, with large communicating endometrial and myometrial collections (blue arrow) through a focal defect as described above with severe thinning of myometrium (pink arrow) suggestive of Hemato-pyometra.
A cavity (blue star) which is communicating with another large myometrial collection (pink star) large T2 hyperintense collection within the endometrial cavity) through a focal defect.
Diffuse adenomyosis in the right horn (yellow arrow) and fibroids in the left horn (brown arrow).")
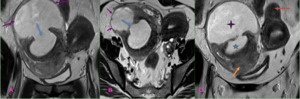
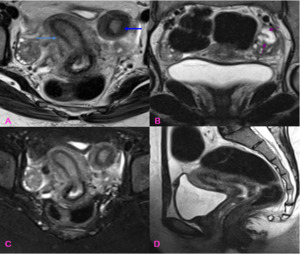
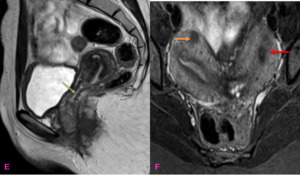
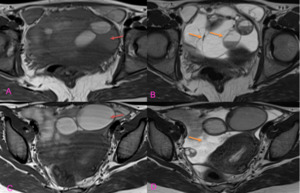
Fig. 5:
T2 axial (B) and coronal images MRI images (A,C) demonstrating Bicornuate...
 and coronal MRI images (E, F) demonstrate a single vaginal and cervical cavity (green arrows) and a communication between the endometrial cavities (red arrow).
T2 sagittal (D) and coronal images MRI images (F) demonstrate diffuse Adenomyosis in the right horn (yellow arrow) and fibroids in the left horn (brown arrow). Features fit into Class IV Mullerian duct anomalies.")
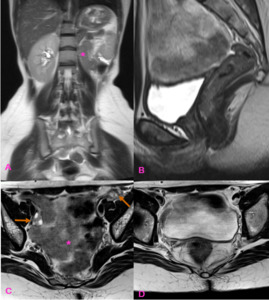
Fig. 6:
T2 sagittal (D) and coronal MRI images (E, F) demonstrate a single vaginal and...
 and coronal (B) STIR axial (C) and T2 sagittal MRI images (D) demonstrate two separate uterine horns (light and dark blue) with the right horn communicating with the cervical canal. No obvious communication between left uterine horn with the right horn or cervical canal. Endometrial cavity seen in the rudimentary horn- Features fitting into Class II b Mullerian duct anomaly.
Mild left Hydrosalpinx (pink arrows).")
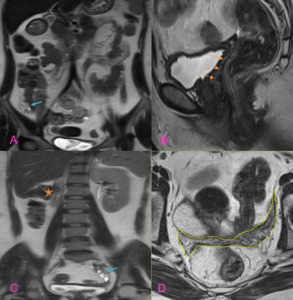
Fig. 7:
T2 axial (A) and coronal (B) STIR axial (C) and T2 sagittal MRI images (D)...
 demonstrates Class III Mullerian duct anomaly - Uterine Didelphys with gravid right horn.
Complete duplication of cervical canal (pink arrows) and uterine horns (yellow arrows) without any communication between them. Right horn is in gravid state with amniotic sac, fetus and posteriorly attached placenta (green star)")
Fig. 8:
30 Year old female with 11 weeks pregnancy and suspected uterine malformation....
 and coronal (B, C, D) MRI images demonstrating Mullerian duct anomaly - class IV b: (Bicornuate unicollis)
Two discrete uterine horns are noted with widened intercornual distance and separate non-communicating endometrial cavities seen in upper part (green arrows).
A submucosal lesion seen in left horn - fibroid (red arrow)")
Fig. 9:
T2 FS axial (A) and coronal (B, C, D) MRI images demonstrating Mullerian duct...
suggesting Mullerian duct anomaly -Bicornuate unicollis -class IV B
Small subserosal (right side, orange arrow) and submucosal (left side, red arrow) in bilateral uterine horns, uterine Fibroids")
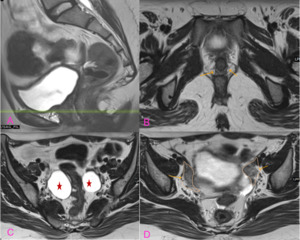
Fig. 10:
Two discrete uterine horns noted with widened intercornual distance with likely...
 and axial (C, D) MRI images demonstrate a Bicornuate Bicollis uterus with duplicated upper cervix (green arrow) s/o Uterus Didelphys (failure of Mullerian duct fusion).
Uterus shows two divergent uterine horns with well-defined endometrium separated by a deep fundal cleft (black star), two separate cervices, duplicated upper vagina (blue arrow).")
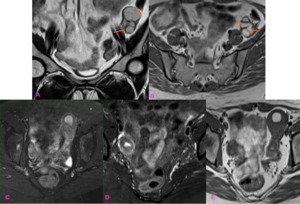
Fig. 11:
T2 coronal (A, B) and axial (C, D) MRI images demonstrate a Bicornuate Bicollis...
 and T1 axial (B) MRI images demonstrates left Haematosalpinx (orange arrows).
STIR FS -axial (C,D) and T1 axial (E) MRI images demonstrates Uterine Didelphyis with left Hematometra.")
Fig. 12:
T2 coronal (A) and T1 axial (B) MRI images demonstrates left Haematosalpinx...
 sagittal (B) axial (C,D) MRI images absent left kidney and absent uterus (star), bilateral ovaries seen (arrows)- Features fitting into Mayer-Rokitansky-Küster-Hauser syndrome (MRKH)")
Fig. 13:
A young patient presented with amenorrhoea; On T2 coronal (A) sagittal (B)...
, axial (B) and coronal (C) MRI images demonstrates two separate uterine cavities (red arrows) and cervical canals (pink arrows). The endometrial cavity is distended and fluid filled.")
Fig. 14:
T2 sagittal (A), axial (B) and coronal (C) MRI images demonstrates two separate...
 and coronal (B, C) MRI images demonstrates a septated right vagina which is distended with fluid within the vaginal cavity (pink arrow) compressing and displacing the left vaginal cavity (yellow arrow). The features are suggestive of uterine Didelphys with imperforated right Hemivagina and Hematocolpos.")
Fig. 15:
T2/T1 FS axial (A, D) and coronal (B, C) MRI images demonstrates a septated...
 and T2 (B, C) axial MRI images demonstrates Unicornuate uterus with small cervix, incompletely visualized, suggestive of cervical agenesis.
Multiple multiloculated cysts (mustard arrows) in the left adnexa suggestive of Endometriotic cysts with non-visualization of left ovary and fallopian tube and mild degree free fluid in the pelvis with thin internal septations, possible menstrual bleed into left ovary and fallopian tube and into the peritoneal cavity (brown arrow)")
Fig. 16:
T1 (A, C) and T2 (B, C) axial MRI images demonstrates Unicornuate uterus with...
 MRI image S5 and coccyx are not visualized, suggestive of partial sacral agenesis and coccygeal agenesis (blue arrow).
Absent vagina (red arrow) on T1 axial MRI image (F). The right ovary is well seen (purple arrow).
The bilateral kidneys were seen on trans-abdominal ultrasound.")
Fig. 17:
On T2 sagittal (E) MRI image S5 and coccyx are not visualized, suggestive of...
 sagittal (B) and axial (D) MRI images demonstrate ill-defined soft tissue extending to the adnexa's (yellow outline) could be hypoplastic uterus/fallopian tubes. Ovaries are seen bilaterally (blue arrow). Upper 1/3rd vagina is well seen (orange arrow). However distal vagina is likely absent. Absent Right Kidney (star) - The features are suggestive of Type IE Mullerian duct anomaly")
Fig. 18:
T2 coronal (A, C) sagittal (B) and axial (D) MRI images demonstrate ill-defined...
, coronal (B, C) and axial (D) MRI images demonstrate absent vagina, uterus, fallopian tube and right kidney (brown star). The bilateral ovaries are well seen (blue arrow).
Features fit into Mayer Rokitansky Kuster Hauser syndrome variety")
Fig. 19:
T2 sagittal (A), coronal (B, C) and axial (D) MRI images demonstrate absent...
, and axial (B,C,D) MRI images demonstrates 2 separate vaginas and 2 ill-defined soft tissue structure in bilateral adnexa's (brown arrow/outline) which could be hypoplastic uteruses, bilateral Hydrosalpinx (star)
Features suggestive of Type 1 Mullerian duct anomaly")
Fig. 20:
T2 sagittal (A), and axial (B,C,D) MRI images demonstrates 2 separate vaginas...