INTRODUCTION
Primary retroperitoneal neoplasms are a diverse group of benign and malignant tumors that arise within the retroperitoneum but outside the major organs.
Of the primary retroperitoneal neoplasms,
70%–80% are malignant in nature,
and these account for 0.1%–0.2% of all malignancies in the body.
One-third of malignant retroperitoneal neoplasms are sarcomas; 15% of all sarcomas originate within the retroperitoneum.
Although computed tomography and magnetic resonance imaging can demonstrate important characteristics of these tumors,
diagnosis is often challenging for radiologists.
Diagnostic challenges include precise localization of the lesion,
determination of the extent of invasion,
and characterization of the specific pathologic type.
ANATOMY OF THE RETROPERITONEAL SPACE
The retroperitoneum is the compartmentalized space bounded anteriorly by the posterior parietal peritoneum and posteriorly by the transversalis fascia.
It extends from the diaphragm superiorly to the pelvic brim inferiorly.
The abdominal retroperitoneum is divided by fascial planes into the anterior and posterior pararenal spaces and the perirenal (or perinephric) space,
Figures 1,
2,
3 and 4.
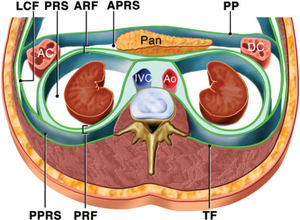
Fig. 1: Drawing of the anatomy of the retroperitoneal spaces at the level of the kidneys. The anterior pararenal space (APRS) is located between the parietal peritoneum (PP) and the an¬terior renal fascia (ARF) and contains the pancreas (Pan), the ascending colon (AC), and the descending colon (DC). The posterior pararenal space (PPRS) is located between the posterior renal fascia (PRF) and the transversalis fascia (TF). The perirenal space (PRS) is located between the anterior renal fas¬cia and the posterior renal fascia. Ao = aorta, IVC = inferior vena cava, LCF = lateroconal fascia
References: Rajiah et al. (2011) "Imaging of uncommon retroperitoneal masses." Radiographics 31.4; 949-976.
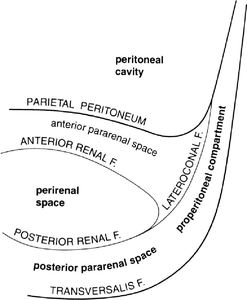
Fig. 2: Diagram of the left retroperitoneal space detailing the fasciae and compartments
References: Burkill et al (2000). "Anatomy of the retroperitoneum." Imaging12.1, 10-20.
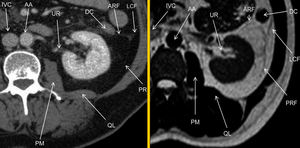
Fig. 3: Computed tomography and Magnetic resonance imaging T2 weighted sequence. Anatomy of the retroperitoneal space.AA abdominal aorta, ARF anterior renal fascia, DC descending colon, IVC inferior vena cava, LCF lateroconal fascia, PRF posterior renal fascia, PM psoas muscle, QL quadratus lomborum muscle, UR ureter.
References: Quaia et al, (2014) "Normal radiological anatomy of the retroperitoneum." Radiological Imaging of the Kidney. Springer Berlin Heidelberg; 75-79.
Compartments
Anterior pararenal space
The anterior pararenal space is confined by the posterior parietal peritoneum anteriorly,
the anterior renal fascia posteriorly,
and the lateroconal fascia laterally.
It contains the ascending and the descending colon (pericolonic component),
the second (descending),
third (transverse),
and fourth (ascending) loops of the duodenum,
and pancreas (pancreaticoduodenal component).
Perirenal space
The perirenal space is confined by the anterior renal fascia (Gerota fascia) and posterior renal fascia (Zuckerkandl fascia),
which together comprise the renal fascia.
It contains the kidneys,
renal vessels,
adrenal glands,
renal pelvis,
proximal ureters,
perirenal lymphatics,
and perirenal fat
Posterior pararenal space
The posterior pararenal space is confined by the posterior renal fascia anteriorly,
by the transversalis fascia posteriorly,
and by the psoas muscle medially.
It continues laterally external to the lateroconal fascia as the properitoneal fat of the abdominal wall.
It almost always contains only fat.
The great vessel space
The great vessel space is the fat-containing region that surrounds the aorta and the inferior vena cava (IVC) and lies anterior to the vertebral bodies and psoas muscles.
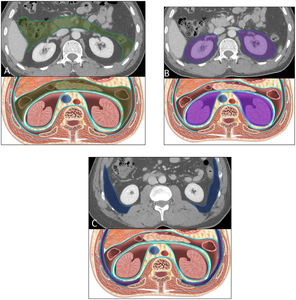
Fig. 4: Retroperitoneal spaces.CECT axial images and corresponding illustrations delineate (A) the anterior pararenal space,(B )perirenal space, and (C) the posterior pararenal space.CECT,contrast-enhanced CT.
References: Osman et al. (2013) "A comprehensive review of the retroperitoneal anatomy, neoplasms, and pattern of disease spread." Current problems in diagnostic radiology 42.5; 191-208.
Summary of Primary Retroperitoneal Masses
Solid retroperitoneal masses may be divided into neoplastic and non-neoplastic categories,
Retroperitoneal cystic masses are uncommon.
They may be divided into neoplastic and non-neoplastic categories (Table 1).
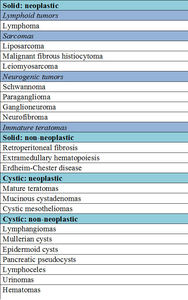
Table 1: Differential diagnosis of primary retroperitoneal masses
References: Scali et al. (2014). "Primary retroperitoneal masses: what is the differential diagnosis?." Abdominal imaging; 1-17.
SOLID NEOPLASTIC
LYMPHOMA
Lymphoma is the most common retroperitoneal malignancy,
accounting for 33% of all primary retroperitoneal masses.
Retroperitoneal lymphomas typically present as well defined para-aortic or pelvic masses,
which demonstrate homogeneous attenuation on non-contrast CT.
They tend to be hypovascular and demonstrate mild homogeneous enhancement on contrast-enhanced CT.
They often appear as a mantle-like mass around the aorta or IVC,
extending between and encasing structures without compressing them,
The aorta and IVC can be anteriorly displaced,
producing the “floating aorta” or “CT angiogram” sign.
NEUROGENIC TUMORS
Retroperitoneal neurogenic tumors constitute 10% to 20% of primary retroperitoneal tumors in adults,
they can originate from the nerve sheath (schwannoma,
neurofibroma,
MPNST),
ganglionic cells (ganglioneuroma,
ganglioneuroblastoma,
neuroblastoma) or from paraganglionic cells (paraganglioma).
Neurogenic tumors are seen commonly along the sympathetic ganglia,
which are located in the para-spinal region,
and in the adrenal medulla or the organs of Zuckerkandl (para-aortic bodies).
Although radiologic features of neurogenic tumors are often overlapped,
predominant or specific CT features are present in each type:
- Paraganglioma (They are hypervascular tumors that enhance briskly).
- Neuroblastoma (Neuroblastoma is the third most common pediatric malignancy,
Two-thirds of neuroblastomas are located in the abdomen,
of which two-thirds of abdominal neuroblastomas are located in the adrenal gland and the remainder in the extra-adrenal retroperitoneum).
- Ganglioneuroblastoma.
- Ganglioneuroma.
- Schwannoma.
- Neurofibroma.
GERM CELL,
SEX CORD,
AND STROMAL CELL TUMORS
Primary extra-gonadal germ cell tumors
Primary extra-gonadal germ cell tumors are rare,
accounting for 1.0–2.5% of germ cell tumors.
A gonadal primary must first be excluded,
since the majority of retroperitoneal germ cell tumors represent metastases
Teratoma
Teratoma accounts for as many as 11% of primary retroperitoneal tumors and is the third most common tumor in the retroperitoneum in children,
after neuroblastoma and Wilms tumor
- Mature teratoma (dermoid cyst) are predominantly cystic.
Calcification (tooth like or well defined) and fat can be seen in 56% and 93% of cases,
respectively. A fat-fluid (sebum) level and chemical shift between fat and fluid are pathognomonic.
- Immature teratoma is less common (<1%),
contains more than 10% undifferentiated tissue,
and is seen in a younger age group (<20 years). Immature teratoma is predominantly solid,
with scattered areas of fat and calcification (coarse and ill defined),
but cystic components are found occasionally.
It may be difficult to distinguish between immature and mature teratomas on imaging alone.
SARCOMAS
Sarcomas are rare neoplasms of mesenchymal origin that account for <1% of all malignancy in adults,
15% of which occur in the retroperitoneum.
Liposarcoma
Liposarcoma is the most common primary retroperitoneal sarcoma and accounts for 40% of cases,
and is the second most common adult soft tissue sarcoma.
Liposarcomas are histologically subdivided into five main subgroups in the order of increasing malignancy: 1) well-differentiated,
2) myxoid,
3) dedifferentiated 4) round cell and 5) pleomorphic liposarcoma.
|
Well differentiated
|
Low metastatic potential;
low-grade histology;
high local recurrence (w100%);
10% eventually dedifferentiate
|
|
Dedifferentiated
|
Features of liposarcoma subtypes
Worst prognosis; calcification
or ossification may be seen (30%)
|
|
Myxoid
|
25% may not contain fat;
pseudocystic appearance
on unenhanced images from the myxoid component;
MFH has similar appearance
|
|
Pleomorphic and round-cell
|
Least common subtype,
aggressive lesions with little or no macroscopic fat
|
|
|
Leiomyosarcoma
Leiomyosarcoma is the second most common retroperitoneal sarcoma,
accounting for 30% of all cases.
Leimyosarcomas are most common in the fifth to sixth decade and have a female predominance.
Leiomyosarcoma is the most common intraluminal venous neoplasm and is the most common primary tumor of the IVC .The finding of a retroperitoneal mass which has both intraluminal and extraluminal components is very suggestive of a leiomyosarcoma.
Malignant Fibrous Histiocytoma (MFH)
MFH is the third most common primary retroperitoneal sarcoma,
accounting for 15% of all cases.
They most commonly occur in the fifth to sixth decade and predominantly affect men.
Imaging features are non-specific and typically demonstrate large,
well-circumscribed soft tissue masses that enhance heterogeneously.
Areas of necrosis and hemorrhage may be seen but are not as extensive as in leiomyosarcomas.
Direct invasion into adjacent organs may occur.
Calcification occurs in up to 20% in a lumpy or ring-like pattern peripherally or a speckled pattern centrally
SOLID NON NEOPLASTIC
RETROPERITONEAL FIBROSIS (RPF)
RPF is a rare collagen vascular disease that is most common in men of the fourth to sixth decades.
The etiology of RPF is idiopathic in two-thirds of cases,
resulting from immune reaction to antigens contained within atheromatous plaques of the abdominal aorta; the remaining one-third of cases are secondary to malignancy,
medications,
aortic aneurysms,
or infections
On unenhanced CT,
retroperitoneal fibrosis is isodense to surrounding muscle.
The normal fat planes surrounding aorta,
inferior vena cava (IVC),
and psoas muscles are obliterated.
Retroperitoneal fibrosis displaces the ureters medially.
Most other conditions in the differential diagnosis result in lateral displacement of the ureters.
In the acute stage of disease,
avid enhancement can be observed in retroperitoneal fibrosis.
During the later stages,
mild or even no enhancement occurs.
On MR imaging,
RPF has low to intermediate T1-signal intensity.
The T2-weighted signal intensity and the enhancement pattern of RPF depend on the activity of the disease.
Cystic lesions
|
Neoplastic cysts
|
Non neoplastic cysts
|
|
Mucinous cystadenoma
|
Cystic lymphangioma
|
|
Cystic mesothelioma
|
Mullerian cyst
|
|
Cystic teratoma
|
Epidermoid cyst
|
|
Cystic change in solid neoplasm
|
Bronchogenic cyst
|
|
Pseudomyxoma retroperitonei
|
Pancreatic pseudocyst
|
|
Perianal mucinous carcinoma
|
Nonpancreatic pseudocyst
|
|
|
Tailgut cyst
|
|
Lymphocele
|
|
Urinoma
|
|
Hematoma
|


 is located between the parietal peritoneum (PP) and the an¬terior renal fascia (ARF) and contains the pancreas (Pan), the ascending colon (AC), and the descending colon (DC). The posterior pararenal space (PPRS) is located between the posterior renal fascia (PRF) and the transversalis fascia (TF). The perirenal space (PRS) is located between the anterior renal fas¬cia and the posterior renal fascia. Ao = aorta, IVC = inferior vena cava, LCF = lateroconal fascia References: Rajiah et al. (2011) "Imaging of uncommon retroperitoneal masses." Radiographics 31.4; 949-976.")
. "Anatomy of the retroperitoneum." Imaging12.1, 10-20.")
 "Normal radiological anatomy of the retroperitoneum." Radiological Imaging of the Kidney. Springer Berlin Heidelberg; 75-79.")
 the anterior pararenal space,(B )perirenal space, and (C) the posterior pararenal space.CECT,contrast-enhanced CT. References: Osman et al. (2013) "A comprehensive review of the retroperitoneal anatomy, neoplasms, and pattern of disease spread." Current problems in diagnostic radiology 42.5; 191-208.")
. "Primary retroperitoneal masses: what is the differential diagnosis?." Abdominal imaging; 1-17.")