Type:
Educational Exhibit
Keywords:
Obstetrics (Pregnancy / birth / postnatal period), Genital / Reproductive system female, Pelvis, MR, Diagnostic procedure, Obstetrics
Authors:
U. S. Umer, S. Alam, A. N. Khan, S. G. Ghaus, S. Gul, S. Gul, H. Abid, A. Safi, K. Nawab; Peshawar/PK
DOI:
10.26044/ecr2019/C-1504
Background
Introduction and Pathophysiology:
Morbidly adherent placenta (MAP) is a severe pregnancy complication that occurs when the chorionic villi abnormally invade the myometrium.
Its pathogenesis is primarily attributed to defective decidualization of the implantation site.
The increasing incidence of morbidly adherent placenta has greatly increased the risk of a possible threat to life1,
2.
The incidence of MAP has risen substantially due to the increased rate of cesarean sections (CS) 3 and previous damage to myometrial wall,
through prior cesarean section is the most important risk factor.
Morbidly adherent placenta remains one of the greatest challenges in modern obstetrics 9. Clinical risk factors include placenta previa and prior uterine surgery,
including CS delivery. Current estimates indicate a 25% to 50% incidence of placenta accreta in patients with placenta previa and prior cesarean delivery.
Types of Morbidly Adherent Placenta:
It has three variants depending on the depth of placental invasion (Figure.1):
- Accreta: The placenta is attached to the myometrium.
- Increta: The placenta extends into the myometrium.
- Percreta: The placenta extends through the entire myometrium and uterine serosa; this variant can lead to the placental attachment to other organs such as the rectum and bladder.
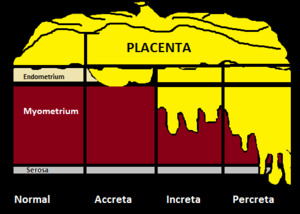
Fig. 1: Diagram of grades of abnormal placental infiltration. (1) Placenta accreta is adherent to the myometrium. (2) Placenta increta invades the myometrium. (3) Placenta percreta extends into or beyond the uterine serosa and may invade any other organ.
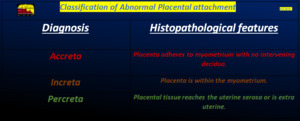
Table 1: Classification of abnormal placental attachment.
Early and systematic detection of abnormal placentation is a crucial step in planning delivery and subsequent management.
Optimal management requires accurate prenatal diagnosis.
Role Of Imaging:
Ultrasonography (USG) and magnetic resonance imaging (MRI) are the modalities for prenatal diagnosis of placenta accreta,
although USG is primary investigation of choice and MRI is used as complementary technique usually reserved for further characterization when USG is inconclusive or incomplete 2.
Reader accuracy and confidence require adherence to MRI examination performance,
image interpretation criteria and awareness of common pitfalls4.
Different MRI techniques and sequences have been studied for accurate detection of morbidly adherent placenta.
This exhibit focuses on the different variants of MAP,
its association with previa and specific imaging findings on MRI.
We would identify new criteria and review established MR criteria for diagnosis of MAP and its correlation with clinical outcome.
The aim of this poster is to provide a primer for radiologists performing MRI for suspected morbidly adherent placenta,
illustrating normal and abnormal findings and diagnostic pitfalls.


 Placenta accreta is adherent to the myometrium. (2) Placenta increta invades the myometrium. (3) Placenta percreta extends into or beyond the uterine serosa and may invade any other organ.")
