ECR 2019 / C-1519

Pulmonary vascular congenital anomalies on MDCT
Congress:
ECR 2019
Poster Number:
C-1519
Type:
Educational Exhibit
Keywords:
Congenital, Structured reporting, Normal variants, Computer Applications-3D, CT-Angiography, CT, Vascular, Pulmonary vessels, Lung
Authors:
U. S. Umer, S. Alam, S. G. Ghaus, S. Gul, A. N. Khan, S. Gul, H. Abid, A. Safi; Peshawar/PK
DOI:
10.26044/ecr2019/C-1519
.")
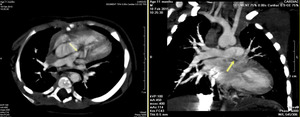
Fig. 1:
Axial MIP-ped image of CT angiogram showing stenosis at origin of left main...

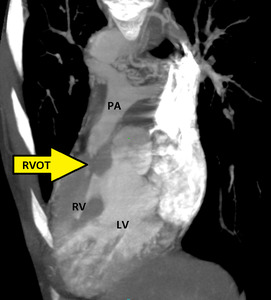
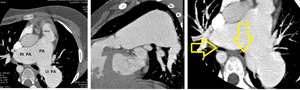
Fig. 2:
Multiplanar CT Angiography images showing Pulmonary stenosis at supravalvular...
 and severe stenosis of right ventricular outflow tract (RVOT) seen (arrow). PA=pulmonary artery, LV=left ventricle, RVOT=right ventricular outflow tract.")
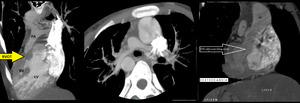
Fig. 3:
Curved MPR CT image of a cardiopulmonary angiogram showing hypertrophy of...

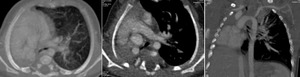
Fig. 4:
Situs inversus with dextrocardia and Tetrology of Fallots. Myltiplanar...

Fig. 5:
Unilateral Pulmonary Agenesis: CT images showing single left pulmonary artery....

Fig. 6:
Pulmonary agenesis. Multiplanar images of a CT angiogram showing complete...
.")
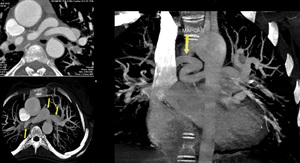
Fig. 7:
Multiplanar CT images of 11 year old girl showing marked aneurysmal dilatation...
. There is secondary left ventricular dilatation and cardiomyopathy.")
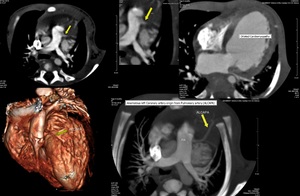
Fig. 8:
Multiplanar images of Cardiac CT scan showing anomalous origin of left coronary...

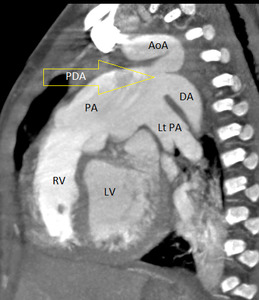
Fig. 9:
3D Volume rendered images from a CT angiogram showing large functional PDA...
. There is coarctation / interrupted aorta variant and PDA is acting as a conduit between arch and descending aorta.RV=right ventricle, LV= left ventricle, PA= pulmonary artery, DA=descending aorta, AoA=aortic arch, LtPA= left pulmonary artery.")
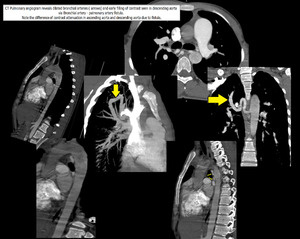
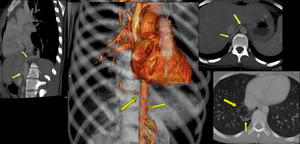
Fig. 10:
Aneurysmal dilatation of pulmonary artery due to a large PDA (arrow). There is...

Fig. 11:
Multiplanar images of CT Pulmonary angiogram showing Bronchial artery -...
")
Fig. 12:
Sequestration. Multiplanar and 3D volume rendered images showing intralobar...

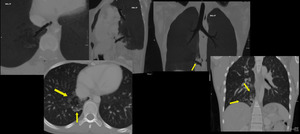
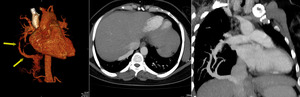
Fig. 13:
Sequestration: Multiplanar lung window images showing intralobar pulmonary...
. Bilateral pulmonary veins are joining to form a single channel posterior to Left atrium of heart, which opens into the right atrium near opening of coronary sinus.")
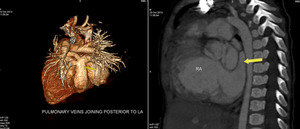
Fig. 14:
TAPVR. 3D volume rendered and sagittal oblique reconstructed image from a CT...

Fig. 15:
SCIMITAR. Partial anomalous pulmonary venous return. Anomalous right lower...
.")
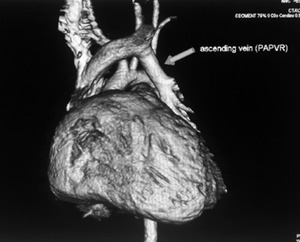
Fig. 16:
PAPVR. Unilateral pulmonary veins have joined to form an ascending channel to...