We have analyzed the imaging,
clinical data,
and postoperative histopathological results of 38 patients with SRMs who underwent radical nephrectomy,
nephron sparing surgery,
or radiofrequency ablation.
In this poster we included the most interesting cases from the analyzed group of patients.
Case 1. 77-yo patient with incidentally finding of SRM sized 16x16x16mm in the central part of right kidney treated with radical nephrectomy (Fig.1).
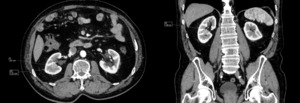
Fig. 1: The measurments of the lesion located in the central part of right kidney.
According to the European Association of Urology guideline [1] elderly and comorbid patients with SRMs have low RCC-specific mortality and significant competing-cause mortality.
The risk of renal failure is much higher in this group of patients.
Active Surveillance is appropriate to initially monitor SRMs,
followed if required by treatment for progression.
Percutaneous Radiofrequency Ablation (RFA) is also a safe method saving renal parenchyma recommended in this group of patients,
but it cannot be used for centrally localized tumors.
The increasingly used ablative technique is Irreversible Electroporation (IRE).
Electroporation is a method based on short pulses of high voltage,
which lead to apoptosis of membranous cell structures.
The recent study by Wender JJ,
Pech M,
Fischbach F et al showed that IRE might be useful for ablation of centrally localized tumors showing complete tumor destruction with the protection of the urine-collecting system [2].
Case 2. 68-yo patient with tumor in left kidney.
Lesion was oversized by a radiologist who also reported the ingrowth in kidney hilum.
Based on this report,
the radical nephrectomy was performed.
In the patomorphological examination tumor size was 38x35x32mm qualified as pT1a clear cell carcinoma (Fig.
2).
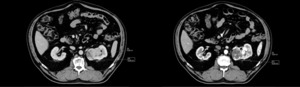
Fig. 2: The oversizing is caused by inclusion of irregular hilar vessels into the tumor size.
The oversizing is caused by inclusion of irregular hilar vessels into the tumor size.
Case 3. The 2 cases of patients with different management according to the similar condition - SRM in a cirrhotic kidney.
The first patient (F,48-yo) is after kidney transplantation due to chronic renal inssuficiency with SRM in the left kidney.
Due to non functioning kidney the management was radical nephrectomy (Fig.
3)
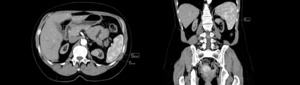
Fig. 3: The measurments of the lesion located in upper pole of left kidney.
In the other patient (M,75-yo) RFA was successfully performed.
According to the contrast enhancement of the kidney,
we suppose that it was hypoplastic,
not cirrhotic.
Applying RFA as a method of choice,
and in this case,
saved the functioning renal parenchyma (Fig.
4).

Fig. 4: The images performed before, during and after RFA. The arrows show the lesion in right kidney. Gas bubbles are present in the examination during RFA due to thermal effect of this method.
Case 4. 58-yo patient underwent radical nephrectomy of the right kidney due to chromophobic cancer and was scheduled for nepfron surgery of left kidney due to clear cell renal cancer.
In follow up study the new lesion was found measuring 35x33x35mm.
The treatment was radical nephrectomy (Fig.
5).
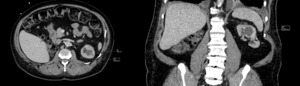
Fig. 5: The measurements of the lesion found in solitary kidney.
Patients with a history of renal cell carcinoma present a higher risk of developing a new lesion. Nephron sparing surgery is preferred over RFA in the management SRMs,
also in patients with solitary kidney [3].
However,
even minimally invasive surgery can lead to renal failure in the group of patients with a risk of life long hemodialysis.
RFA preceded with biopsy is a safe,
increasingly used method with successful results and minor complications [4,5,6].
It should be considered in planning of tumor treatment.
Case 5. The 75 year old patient underwent chest CT.
Kidneys were partly seen in the examination.
In the right kidney there was a small,
well circumscribed lesion,
showing enhancement after intravenous contrast administration,
measuring 17x16x14mm.
In the left kidney a lesion with fatty tissue,
accumulation,
typical of angiomyolipoma,
is seen (Fig.
6).
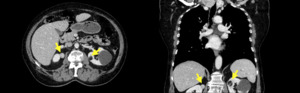
Fig. 6: The images show poor-fat angiomyolipoma and typical angiomyolipoma with dominant fat accumulation.
The main problem in this case was the lack of biopsy prior to surgery.
Richard PO,
Jewett PA,
Bhatt JR et al showed that performing biopsy leads to avoiding surgical treatment even in 26% of patients due to the benign character of lesions [7]. According to the European Association of Urology percutaneous renal tumor biopsies should be performed to obtain the histology of radiologically indeterminate renal masses,
to select patients to active surveillance or before ablative treatments [1].
Case 6. 69-yo patient with hemolytic anemia underwent abdominal CT.
The study showed exophytic,
irregular lesion in the right kidney.
NSS was performed (Fig.
7).
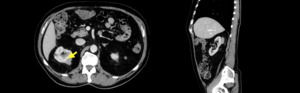
Fig. 7: The arrow shows discrete infiltration of the tumor to the renal parenchyma.
The histopathological diagnosis was marginal zone B cell lymphoma,
which should be treated with systemic treatment as standard.
The biopsy performed prior to the treatment could enable the choice of standard treatment first.
