The abdomen is the third most commonly injured region in trauma,
after the head and extremities.
Splenic injuries are the most common injury in blunt abdominal trauma,
followed by liver injuries and bowel/mesenteric injuries.
Bowel and mesenteric injuries are relatively uncommon,
being detected in 1-5% of patients with blunt abdominal trauma at laparotomy.
It may be a diagnostic challenge for the radiologist due to the subtle imaging findings,
presence of multiple concurrent injuries or injury of multiple bowel segments.
Delayed diagnosis of bowel and mesenteric injuries results in increased morbidity and mortality due to HEMORRHAGE or SEPSIS.
INJURY MECHANISMS:
The most common cause is motor vehicle accident.
Mechanisms = crush,
shear and burst.
-Direct force crushing the gastrointestinal tract
-Rapid deceleration producing shearing force between fixed and mobile portions of the tract
-Sudden increase in intraluminar pressure with bursting injuries
LOCATION:
The small intestine is more frequently injured than the colon and the commonest injury is a perforation in the anti-mesenteric border of the small intestine.
The three most common locations are:
-PROXIMAL JEJUNUM near the ligament of Treitz
-DISTAL ILEUM near the ileocecal valve
-MULTIPLE SITES of injury
-Others: duodenum (specially 2nd and 3rd portions),
colon (transverse and sigmoid colon are more vulnerable),
stomach.
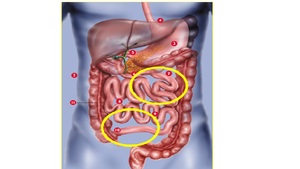
Fig. 1: The most common locations of bowel trauma are: PROXIMAL JEJUNUM and DISTAL ILEUM (yellow circles).
References: http://www.genesishealth.com/care-treatment/weight-management/expect/digestive_diagram/
DIAGNOSIS:
Pain from peritoneal irritation is nonspecific and it may not be present when the patient is initially evaluated.
Furthermore,
it is common that there is a concomitant trauma which make abdominal assessment difficult,
such as head or spinal cord trauma,
and the results of a physical examination may not be reliable.
- Diagnostic peritoneal lavage:
High sensitivity for the detection of hemoperitoneum,
but there are some disadvantages: it is not reliable for the assessment of retroperitoneal injuries,
bowel perforation may be missed which the diagnostic procedure is performed soon,
it carries some risk like any invasive procedure,
and it compromises the interpretation of the CT (fluid and air may be present in the peritoneal cavity as a result of lavage).
Nowadays it is not applied in practice.
High sensitivity for the detection of free intra-abdominal fluid.
Disadvantages: it does not identify source of bleeding,
assess the retroperitoneum,
or detect viscera injuries.
Useful diagnostic test in HEMODYNAMICALLY UNSTABLE emergency patients (FAST = Focused assessment with sonography for trauma)
Diagnostic test of choice for the evaluation of blunt abdominal trauma in HEMODYNAMICALLY STABLE patients. Sensitivities of 69%–95% and specificities of 94%–100% for the diagnosis of bowel and mesenteric injuries,
with direct and indirect imaging findings essential for making a timely diagnosis and improving patient outcomes.
It is not usual to identify direct findings of bowel-mesenteric injury by CT,
and findings may not be present when the patient is initially evaluated.
If new symptoms= repeat CT.
MAIN GOAL = to distinguish significant injuries (requires surgical intervention) vs non-significant injuries (conservatory management).

.
References: http://www.genesishealth.com/care-treatment/weight-management/expect/digestive_diagram/")