1- CT PROTOCOL
1.1 THE MOST COMMON SITUATION:
- Intravenous nonionic contrast material = 300 mI/ml,
1,5-2 ml/kg administered intravenously at a rate of 3 ml/sec.
- One sequence (PORTAL VENOUS PHASE) with a scanning delay of 70 sec.
after contrast injection.
- NO oral contrast material.
In many institutions,
administration of oral contrast material has been routine.
However,
many investigators from multiple institutions have shown that administration of oral contrast material is not necessary in the setting of blunt abdominal trauma.
Reasons:
- ADITIONAL TIME = delayed diagnosis and treatment
- RISK of aspiration and vomiting
- Difficulties in intestinal wall assessment with oral contrast material
- No difference in the accuracy of CT performed with or without oral contrast material for the detection of blunt bowel and mesenteric injury
1.2 If we suspect active bleeding,
we perform two scan sequences (arterial and portal venous phase,
with a bolus tracking method).
1.3 If we suspect urinary track injury,
or we would like to illustrate the severity of hemorrhage more clearly,
we perform delayed phase images = After the first CT scan,
we review the images in real time and decide if additional delayed phase images should be obtained.
2- CT FINDINGS ASSOCIATED TO BOWEL AND MESENTERIC INJURY.
MAIN GOALS:
-to identify the injury
-to distinguish significant injuries (surgery management) vs non-significant injuries:
2.1) Bowel injury:
a) IS THERE A BOWEL INJURY?
-Discontinuous bowel wall / laceration (100% specific,
low sensitivity of 10%).
It is the most specific sign of bowel injury.
-Extraluminal spillage of enteric contents
-Oral contrast leak
-Evidence of bowel infarct
-Free air
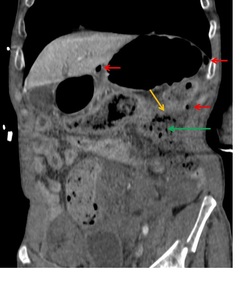
Fig. 2: 56 yo man suicide jumper. Abdominopelvic CT scan with intravenous contrast material (coronal) showing direct findings of bowel injury: Free air (red arrows). Extraluminal spillage of enteric contents (green arrow). Discontinuous bowel wall (yellow arrows). Other findings: pelvic fracture.
-Abnormal bowel wall enhancement:
->Hyperenhancement due to presence of blood,
due to hypoperfusion complex (homogeneous mucosal enhancement that involves a long segment of bowel and is usually associated with other findings of hypovolemic shock) or due to bowel ischemia particularly after reperfusion from an arterial injury (focal mucosal hyperenhancement of the bowel).
->Hypoenhancement due to devascularization,
90% specificity,
10% sensitivity).
-Focal bowel wall thickening >3 mm (eccentric o concentric): specificity 90%,
sensitivity 60%.
This finding is more specific in the large bowel.
More difficult to assess in small bowel: it is often artifactual from inadequate distention,
and when real it is often dismissed abnormal focally thickened bowel wall as normal.
When diffuse small-bowel wall thickening of more than 10 mm is seen = is atypical for contusion and may result from edema secondary to systemic volume overload or to shock bowel.
Additional CT findings of hypovolemic shock complex may also be seen,
such as a flattened inferior vena cava,
narrow calibre aorta, dense renal cortical enhancement and adrenal hyperenhancement.
These findings (abnormal wall enhancement and focal bowel wall thickening) could be due to mesenteric injury with vascular compromise.

Fig. 3: Same case. Axial angio-CT showing indirect findings of bowel injury: Hyperenhancement and thickening of jejunum (yellow arrows). Free fluid (blue arrow).
-Focal pneumatosis: This very uncommon finding may indicate full-thickness involvement that requires surgery.
-Free fluid
-Mesenteric fat stranding
-Peritonitis: enhancement of the peritoneum after intravenous contrast) a not diagnosed bowel laceration could lead to lethal peritonitis !!
b) IS THE INJURY SIGNIFICANT OR NONSIGNIFICANT?
-Complete tear of the wall: laceration is an uncommon finding on CT due to the small size,
we usually identify direct findings of bowel injury (free air,
spillage of enteric contents)
-Incomplete tear that extends to but does not involve the mucosa
-Bowel infarction: Hypoenhancement of a segment of the wall = important devascularization
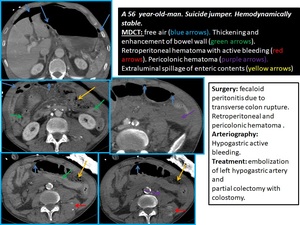
Fig. 4: MAJOR BOWEL AND MESENTERIC INJURIES
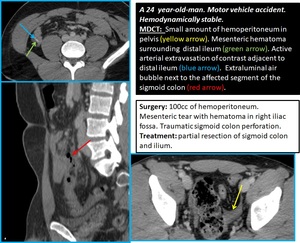
Fig. 5: MAJOR BOWEL AND MESENTERIC INJURIES
-Hematoma
-Tear limited to the serosa
2.2) Mesenteric injury:
a) IS THERE A MESENTERIC INJURY?
-Extravasation of contrast or abrupt termination of mesenteric vessels (disruption of the mesentery): best appreciated on the coronal or sagittal reformatted images.
-Mesenteric hematoma

Fig. 6: 46 yo woman. Traffic collision. Patient hemodynamically unstable. FAST: large amount of free fluid. She was taken to operating room: jejunum tear, resection with laterolateral anastomosis. Postoperative angio-CT (axial and coronal): mesenteric hematoma (green arrow) with active bleeding (blue arrow).
-Free fluid
-Mesenteric fat stranding: sensitivity and specificity for acute mesenteric injury of 70% and 40-90%,
respectively.
It is a hazy appearance and increased attenuation in the mesentery.
The finding is suggestive of mesenteric hematoma or contusion and may be seen either with or without an associated bowel injury.
Differential diagnosis: mesenteric panniculitis (which is better defined and is associated with flat lymph nodes).

Fig. 7: Mesenteric fat stranding. No ohter findings.
TO KEEP IN MIND= These indirect findings could be present due to bowel injury alone,
to mesenteric injury alone,
or due to bowel+mesenteric injury.
b) IS THE INJURY SIGNIFICANT OR NONSIGNIFICANT?
-Active mesenteric bleeding
-Disruption of the mesentery
-Mesenteric injury associated with bowel ischemia
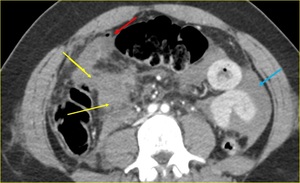
Fig. 8: Devascularization of large segment of small bowel on the right flank (yellow arrows) due to mesenteric avulsion (mesenteric active bleeding seen during the surgery, controlled with packing). Tiny amount of free air (red arrow) due to jejunum laceration (the patient has undergone resection and latero-lateral anastomosis). Large amount of hemoperitoneum (blue arrow).
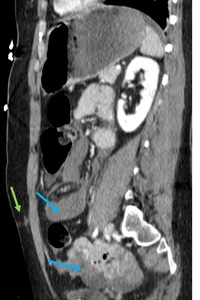
Fig. 9: Same case on sagittal. Seat-belt injury (green arrow). Hemoperitoneum (blue arrows).
-Mesenteric hematoma
3- IS IT A PITFALL?
3.1 FREE AIR:
Sensibility 50%.
High specific for bowel injury (specificity of 95%) but not 100%!!.
a) CAUSES OF EXTRALUMINAL AIR:
-Bowell perforation
-From traumatic injury of the chest = pneumothorax,
pneumomediastinum
-Diaphragmatic injury
-Intraperitoneal bladder rupture when a Foley catheter is present
-Iatrogenic: chest tube placement
b) LOCATION: The location of extraluminal air may be useful in determining the location of the bowel injury.
-Intraperitoneal free air = injury from the first portion of the duodenum,
jejunum,
ileum,
cecum,
transverse colon,
sigmoid colon,
and upper part of the rectum: Gas from ruptured bowel commonly accumulates deep to the anterior abdominal wall,
anterior peritoneal surface of the liver and near the perforation site
-Free air in the retroperitoneum = injury in the second to fourth portions of the duodenum,
the ascending colon,
or the descending colon.
-Other sites: the porta hepatis,
mesenteric veins,
and the portal vein
c) TO KEEP IN MIND/RECOMMENDATION: If there are extraluminal air and other bowel/mesenteric injury finding (seat-belt-sign,
free fluid,
bowel wall thickening,
fat stranding…) = highly predictive of bowel injury =warrants exploration
3.2 FREE FLUID:
Not specific for bowel/mesenteric injury (sensitivity 95%,
specificity 20%).
a) CAUSES OF FREE FLUID
- Bleeding from solid viscera
- Bowel/mesenteric injury = THE MOST SENSITIVE SIGN OF BOWEL INJURY is the presence of free fluid.
- Aggressive intravenous hydration / fluid overload
- Ascites (heart failure,
hepatitis,
malignant ascites…)
- Small amount of free fluid in pelvis = physiological finding in premenopausal females.
Also it could be present in males (3%) and postmenopausal females in the absence of any appreciable abdominal injury.
b) TO KEEP IN MIND/RECOMMENDATIONS:
- Free intraperitoneal fluid could be the only finding of bowel/mesenteric injury= in the absence of solid viscera injury,
we should suspect a bowel/mesenteric injury = a follow-up CT in 8h is recommended = if there is an increase of free fluid and pathological abdominal exploration,
a surgical management is justified.
- If hyperattenuating free fluid = suspect bowel/mesenteric injury.
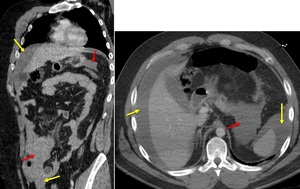
Fig. 10: 53 yo woman who suffered a car accident, hemodynamically stable. Contrast CT on coronal and axial: large amount of perihepatic, perisplenic, mesenteric and pelvis hyperattenuating free fluid, in keeping with hemoperitoneum (yellow arrows). Fat stranding and mesenteric hematoma without active bleeding (red arrows). Surgery: large amount of hemoperitoneum and mesenteric hematoma, no bowel injury. Treatment: drainage of peritoneal fluid and saline lavage.
4- TREATMENT:
4.1 NON-SURGICAL MANAGEMENT:
a) INDICATIONS:
-Patient with questionable findings at the initial CT: clinical observation is recommended.
-Patient with a high risk of bowel or mesenteric injury: repeat CT of the abdomen and pelvis in 12-24 h
-If shock bowel suspected,
repeat CT of the abdomen and pelvis after appropriate resuscitation,
for demonstrate improvement in the appearance of the bowel and mesentery
-Sign of non-significant injury on CT: can be managed no surgically.
b) MANAGEMENT:
Observation + prophylactic antibiotics +/- follow-up CT:
4.2 SURGICAL MANAGEMENT:
a) INDICATIONS:
-Sign of significant injury on CT
- signs of peritonitis
- uncontrolled hemorrhage
- deterioration of the patient’s clinical condition
- substantial hemoperitoneum
b) MANAGEMENT:
The surgeon’s primary goal becomes “damage control” = controlling any hemorrhage and repairing any apparent hollow-organ injuries.
Exploratory laparotomy + drainage of septic peritoneal fluid and wound saline lavage + :
-Simple closure = for single perforation of the small intestine,
-More extensive injuries such as multiple perforations and gangrene from mesenteric injuries = resection and anastomosis.
-Large bowel injuries (particularly in the left colon) = creation of stoma.
Mortality rates quoted from blunt intestinal trauma range from 10-30%.

 showing direct findings of bowel injury: Free air (red arrows). Extraluminal spillage of enteric contents (green arrow). Discontinuous bowel wall (yellow arrows). Other findings: pelvic fracture.")
. Free fluid (blue arrow).")


: mesenteric hematoma (green arrow) with active bleeding (blue arrow).")

 due to mesenteric avulsion (mesenteric active bleeding seen during the surgery, controlled with packing). Tiny amount of free air (red arrow) due to jejunum laceration (the patient has undergone resection and latero-lateral anastomosis). Large amount of hemoperitoneum (blue arrow).")
. Hemoperitoneum (blue arrows).")
. Fat stranding and mesenteric hematoma without active bleeding (red arrows). Surgery: large amount of hemoperitoneum and mesenteric hematoma, no bowel injury. Treatment: drainage of peritoneal fluid and saline lavage.")