Aspiration
Aspiration is the most common lung injury resulting from illicit drug use and usually is related to sedative abuse,
particularly opiates. The risk of aspiration depends on the degree of central nervous system depression and the resultant impairment of normal protective mechanisms. The extent of injury depends on the content and volume of aspirate. Aspiration my clear spontaneously or can progress to infectious pneumonia,
lung abscess,
and empyema. Sepsis and acute respiratory distress syndrome can ensue and are associated with high mortality.
Key imaging findings
- Bibasal and peribronchial consolidation
- Small centrilobular nodules and tree-in-bud opacities
- Bronchial wall thickening and endobronchial debris
- Gravitational dependent distribution
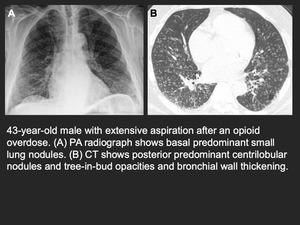
Fig. 1: Opioid-associated aspiration
References: Chest Radiologists Collaborative - Madison/US 2019
Infections
Community-Acquired Pneumonia
The incidence of community-acquired pneumonia (CAP),
including tuberculosis,
is more common in users of illicit drugs,
not only because of lower socioeconomic conditions but also as a result of impaired immunity. Coexistent HIV infection in many IV drug users also increases risk for CAP. Substance abuse has been linked to higher rates of intensive care unit admission and mechanical ventilation,
while IV drug use increases risks of parapneumonic effusion and empyema.
Further complicating matters is the higher association of illicit drug use with antibiotic resistant organisms including methicillin-resistant Staphylococcus aureus.
Key imaging findings
- Single or multiple foci of lung consolidation
- Cavitation with necrotizing infection including tuberculosis
- Nodules of varying sizes and tree-in-bud opacities
- Associated small pleural effusions or empyema
Opportunistic Infections
Marijuana for medical use has increased in popularity and is legal in many countries and U.S.
states.
Patients with cancer may use marijuana to ameliorate side effects from chemotherapy or to help with cancer-related pain.
Patients with other chronic illnesses such as Crohn disease also use marijuana to mitigate symptoms. Because these patients may have varying degrees of immunosuppression,
they are at increased risk of opportunistic infections. In particular,
pulmonary aspergillosis as been described in immunosuppressed patients smoking marijuana.
In these cases,
a cellular bronchiolitis is most common,
characterized by well-defined centrilobular nodules and tree-in-bud opacities on CT.
Key imaging findings
- Same as community-acquired infections
- Diffuse or patchy ground-glass opacity (especially Pneumocystis)
- Nodules with surrounding ground-glass opacity (especially Aspergillus and Nocardia)
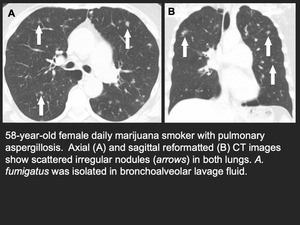
Fig. 2: Marijuana-associated aspergillosis
References: Chest Radiologists Collaborative - Madison/US 2019
Bloodborne Infections
IVDU patients are at high risk of bloodborne infections from contaminated drugs,
unclean syringes and needles,
and skin flora. Thoracic complications of these infections include skin,
soft tissue,
and joint abscesses; endocarditis; infected (mycotic) pseudoaneurysms; and pulmonary septic emboli.
Spinal osteomyelitis-diskitis can also result from IVDU.
Key imaging findings:
- Peripheral nodules with varying degrees of cavitation and surrounding ground-glass opacity (septic emboli)
- Pulmonary and systemic arterial saccular outpouchings (mycotic aneurysms)
- Cardiac vegetations
- Osteolysis and paraspinal collections (osteomyelitis-diskitis)
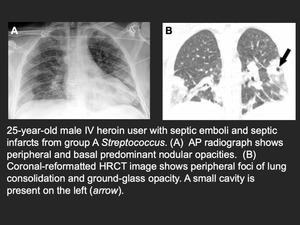
Fig. 3: Septic emboli from IV drug use
References: Chest Radiologists Collaborative - Madison/US 2019
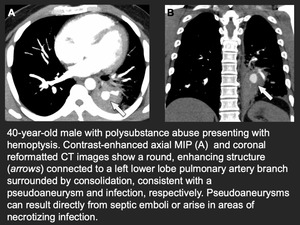
Fig. 4: Mycotic aneurysm
References: Chest Radiologists Collaborative - Madison/US 2019
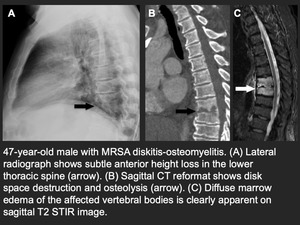
Fig. 5: Diskitis-osteomyelitis from IV drug use
References: Chest Radiologists Collaborative - Madison/US 2019
Inhalational Injury
Inhalation of illicit drugs can result in a variety of lung responses ranging from bronchospasm to diffuse alveolar hemorrhage. Determining the exact cause of lung injury can be difficult because drugs are often mixed with other substances that can can promote airway injury. Acute lung injuries include organizing pneumonia,
eosinophilic pneumonia,
and diffuse alveolar damage. Some patients may develop hypersensitivity pneumonitis from repeated exposures.
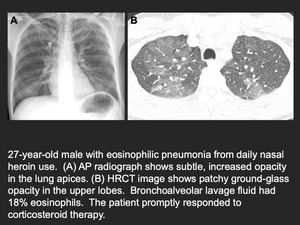
Fig. 6: Eosinophilic pneumonia from heroin
References: Chest Radiologists Collaborative - Madison/US 2019
Similar to injury from intravenous injection of illicit drugs,
chronic lung disease can develop from inhaled particles such as talc,
which may contaminate marijuana or crack-cocaine.
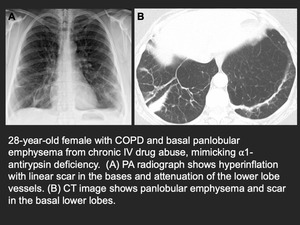
Fig. 7: Basal predominant panlobular emphysema from chronic IV drug use
References: Chest Radiologists Collaborative - Madison/US 2019
Barotrauma can complicate inhalational drug use,
typically resulting from intense inhalation against a closed glottis or Valsalva maneuver with the intent to maximize the amount of drug absorption. Patients usually present with chest pain or shortness of breath from pneumothorax or pneumomediastinum. When severe,
subcutaneous gas and pneumorrhachis can develop. Pneumothorax may require tube thoracostomy.
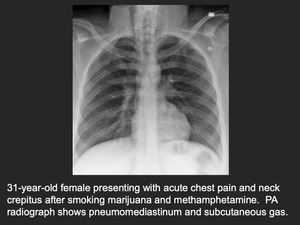
Fig. 8: Barotrauma from smoking marijuana and methamphetamine
References: Chest Radiologists Collaborative - Madison/US 2019
Acute Lung Injury
Noncardiogenic Pulmonary Edema
Noncardiogenic pulmonary edema (NCPE) develops in nearly all fatal cases of opioid overdose and can occur in up to 50% of patients overdosing on heroin. The existence and mechanism of NCPE have been extensively debated in the literature with injury causing leaky pulmonary capillaries as the likely cause. The increased use of naloxone to reduce the CNS depressive effects of opioid overdose may also have an effect on the lungs. Researchers postulate that a rapid increase in sympathetic nervous system activity after apnea reversal may lead to pulmonary edema.
Key imaging findings
- Bilateral diffuse or patchy consolidation and ground-glass opacity
- Rapid development and evolution
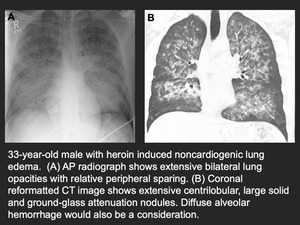
Fig. 9: Opioid-induced noncardiogenic pulmonary edema
References: Chest Radiologists Collaborative - Madison/US 2019
Crack Lung
“Crack lung” is an acute pulmonary syndrome that develops up to 48 hours after smoking crack or free-base cocaine. Patients typically present with fever,
shortness of breath,
hypoxemia,
and hemoptysis.
Histopathologically,
“crack lung” is characterized by diffuse alveolar damage and hyaline membranes. Occasionally,
superimposed eosinophilic pneumonia is present,
usually diagnosed by bronchoalveolar lavage.
Key imaging findings
- Bilateral diffuse or patchy consolidation and ground-glass opacity
- Scattered spared lobules on CT
- Rapid development and evolution
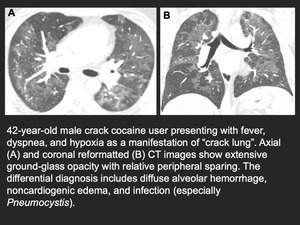
Fig. 10: Crack lung
References: Chest Radiologists Collaborative - Madison/US 2019
Cannabinoid-Associated Lung Injury
Currently,
there is no strong evidence linking the casual recreational use of marijuana to chronic lung disease such as pulmonary fibrosis and COPD. Studies to date have been inconclusive with respect to heavier users and are often confounded by tobacco use,
socioeconomic factors,
and self-reporting biases.
However,
the risk of lung cancer does increase with marijuana smoking and is related to cummulative joint-years of use.
Additionally,
regular marijuana smoking can impair alveolar macrophage function,
leading to increased risk of infection.
Synthetic cannabinoids are more potent than marijuana and are sprayed onto plant leaves to simulate marijuana. While not widely reported,
one small case series showed diffuse airway-centric lung injury characterized predominantly by organizing pneumonia.
Key imaging findings
- Diffuse,
centrilobular nodules and tree-in-bud opacities typical of cellular bronchiolitis
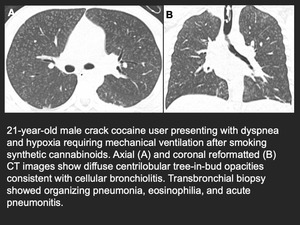
Fig. 11: Organizing pneumonia from synthetic cannabinoid use
References: Chest Radiologists Collaborative - Madison/US 2019
E-Cigarettes / Vaping
Although cigarette smoking rates continue to decline in North America and parts of Europe,
the number of people smoking electronic cigarettes (e-cigarettes) or “vaping” has increased,
especially in younger individuals.
E-cigarettes are marketed as a “safer” alternative to regular tobacco cigarettes,
providing the same physiologic effects of nicotine without exposure to the many known toxins found in conventional cigarettes.
However,
regulation of e-cigarettes by government authorities has been looser than other tobacco products.
Studies have found a variety of known toxins in many e-cigarette compounds,
including diacetyl,
which has been linked to constrictive bronchiolitis.
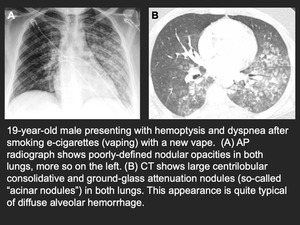
Fig. 12: Diffuse alveolar hemorrhage from smoking electronic cigarette (vaping)
References: Chest Radiologists Collaborative - Madison/US 2019
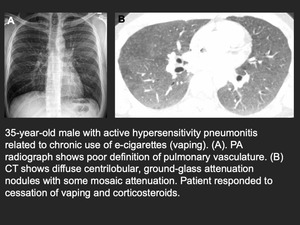
Fig. 13: Vaping-induced hypersensitivity pneumonitis
References: Chest Radiologists Collaborative - Madison/US 2019
Cardiovascular and Pulmonary Vascular Disease
Excipient Lung Disease and Foreign Body Reactions
A variety of insoluble particles,
called excipients,
are used in pharmaceutical manufacturing to bind the active agent into a pill or tablet for oral administration. Additionally,
insoluble particles such as talc,
sand,
glass beads,
microcrystalline cellulose,
and cornstarch are surreptitiously mixed with illicit drugs to increase weight and volume. With repeated intravenous injection of crushed tablets and impure solutions,
these particles can accumulate in the pulmonary vasculature leading to foreign body granulomatous inflammation and vasculitis. Progressive lung injury can cause more widespread damage including fibrosis,
emphysema,
and chronic interstitial inflammation.
Key imaging findings
- Diffuse tiny nodules reflecting pulmonary arteriolar injury and vasculitis (acute or subacute disease)
- Parenchymal destruction and scar (chronic disease)
- Masslike consolidation with high attenuation (talc)
- Right heart dilation,
pulmonary artery enlargement,
or both reflecting elevated right heart pressures
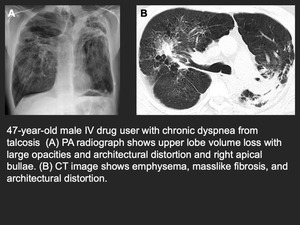
Fig. 14: Talcosis from chronic IV drug abuse
References: Julie Takasugi, MD - Seattle/US
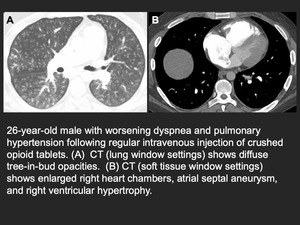
Fig. 15: Excipient lung disease and pulmonary hypertension from IV injection of crushed opioid tablets
References: Chest Radiologists Collaborative - Madison/US 2019
Methamphetamine-Associated Pulmonary Artery Hypertension and Cardiomyopathy
Pulmonary artery hypertension can also develop from chronic methamphetamine use.
In comparison to patients with idiopathic PAH,
methamphetamine-associated PAH (Meth-APAH) patients have worse five-year survival,
functional status,
right heart dysfunction,
and exercise capacity.
Key imaging findings
- Central and peripheral pulmonary arterial enlargement
- Right heart chamber enlargement and right ventricular dilation
- Mosaic attenuation
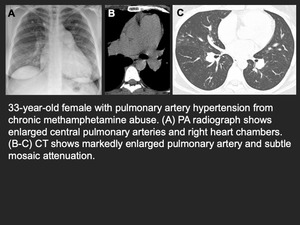
Fig. 16: Pulmonary artery hypertension from chronic methamphetamine abuse
References: Chest Radiologists Collaborative - Madison/US 2019
Methamphetamine abuse has also been linked to cardiomyopathy,
leading to severe heart failure and depressed cardiac function.
The degree of reversibility is linked to the extent of myocardial fibrosis.
Cardiac function can also improve with cessation of methamphetamine use.
Continued abuse leads to progressive heart failure and worse outcomes.
Key imaging findings
- Left ventricular dilation
- Ventricular dyskinesia (Fig. 18)
- Delayed gadolinium enhancement
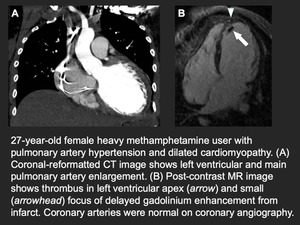
Fig. 17: Dilated cardiomyopathy and pulmonary artery hypertension from heavy methamphetamine abuse.
References: Chest Radiologists Collaborative - Madison/US 2019
Acute coronary syndrome
Acute coronary syndrome has been linked to cocaine use and can result in acute myocardial infarction in patients with few or no risk factors.
Key imaging findings
- Decreased myocardial perfusion
- Cardiac dysmotility
- Cardiogenic lung edema
- Pleural effusion
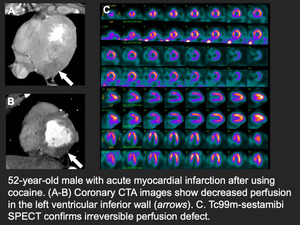
Fig. 19: Cocaine-induced acute myocardial infarction
References: Chest Radiologists Collaborative - Madison/US 2019





 References: Chest Radiologists Collaborative - Madison/US 2019")


