ECR 2019 / C-1661
New images in the evaluation of the inferior vena cava: state of the art
Congress:
ECR 2019
Poster Number:
C-1661
Type:
Educational Exhibit
Keywords:
Veins / Vena cava, Vascular, Abdomen, MR-Angiography, CT-Angiography, Image manipulation / Reconstruction, Computer Applications-3D, Education and training
Authors:
M. F. P. Pereira1, E. C. Raimundo1, L. D. P. G. D. Farias2, D. C. Menezes1, I. S. Faé1, M. D. O. M. Hans1, M. V. Galon1, A. F. Pedri1, M. D. S. Guedes1; 1São Paulo/BR, 2São Paulo, SP/BR
DOI:
10.26044/ecr2019/C-1661
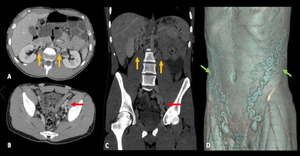
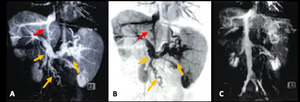
 shows pelvic (red arrows), retroperitoneal (yellow arrows) and abdominal wall varicose veins (green arrows), without characterize IVC in a 19 years old male patient on evaluation for acute inflammatory abdomen reporting of varicose veins in the lower limbs and deep venous thrombosis (DVP). Aorta (black arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
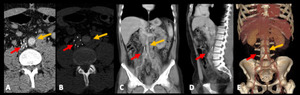
Fig. 4:
IVC ABSENCE. MDCT (A and B – axial, C – coronal, D – 3D reconstruction)...
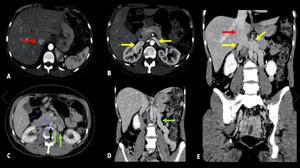
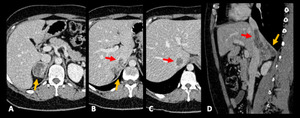
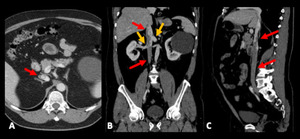
 shows intrahepatic IVC (red arrow), renal veins (yellow arrow) without characterize infrarenal IVC (blue circle), also presenting retroperitoneal varicose veins (green arrows) . Aorta (black arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 5:
INFRARENAL IVC ABSENCE. MDCT (A - C – axial, D and E – coronal) shows...
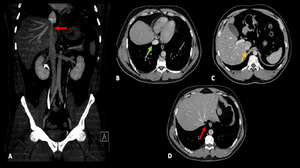
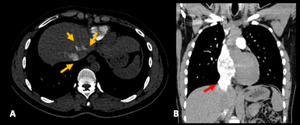
 shows hipoplasia of intra-hepatic segment of the IVC (red arrow) in a 37 years old female patient on evaluation for abdominal pain. Note the relation between the calibers in the vascular segments before (green arrow) and after (yellow arrow) the hypoplastic segment. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 6:
HYPOPLASIA OF THE INTRA-HEPATIC SEGMENT OF THE IVC. MDTC (A – coronal MIP, B...

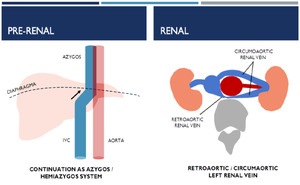
Fig. 7:
PRE-RENAL AND RENAL
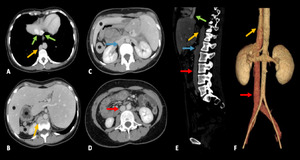
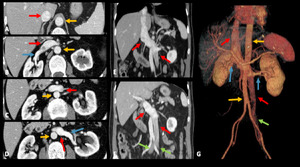
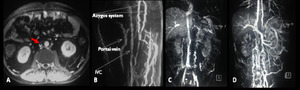
 shows the absence of the hepatic segment of the IVC and the orientation of the IVC (red arrow) for the retrocural aspect (blue arrow) and following continuation with the azygos / hemiazygos system (yellow arrow) in a 29 years old female patient on evaluation for abdominal pain. The hepatic veins drain directly into the right atrium (green arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 8:
CONTINUATION OF THE SUPRARENAL IVC AS THE AZYGOS/ HEMIAZYGOS VEIN. MDTC (A to D...
 shows left renal vein (yellow arrow) between aorta (asterisk) and vertebral body in a 62 years old patient with recurrent abdominal pain in the left flank. Note the white dashed path in posterior and anterior view (D and E). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 9:
RETROARTIC LEFT RENAL VEIN. MDTC (A –oblique axial MIP, B – oblique axial,...
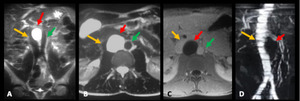
 shows accessory left renal vein (yellow arrow) which drains the lower renal pole, has a posterior pathway to the aorta (asterisk) and the other left renal vein with an anatomical path (green arrow) anterior to the aorta. Notice the narrowing of the accessory left renal vein between the aorta and the vertebral body. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 10:
CIRCUMAORTIC LEFT RENAL VEIN. Angiotomography (A – oblique axial, B –...

Fig. 11:
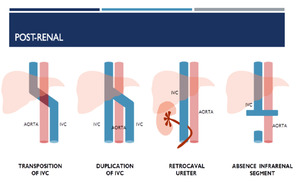
POST-RENAL
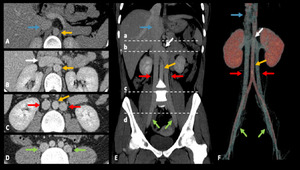
 shows that the IVC (red arrow) ascends to the left of the aorta (yellow arrow) after the confluence of the common iliac veins (green arrow) crossing to the right side at the level of drainage renal veins (blue arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 12:
TRANSPOSITION OF IVC/ LEFT IVC. MDTC (A to D - axial, E and F - coronal, and G...
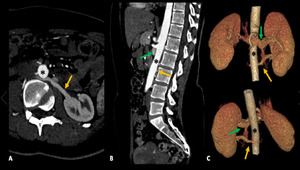
 shows the iliac venous confluence (yellow arrow) posterolateral to the left common iliac artery with ipsilateral ascending path and continuation to the retrocural azygos/ hemiazygos system (red arrow). The azygos/ hemiazygos system drain in the right atrium with superior vena cava (SVC) (purple arrow).
Note the retroaortic pathway of the right renal vein (white arrow) and that the hepatic veins drain directly into the right atrium (blue arrow). Aorta (green arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 13:
TRANSPOSITION OF IVC/ LEFT IVC CONTINUING WITH AZYGOS/ HEMIAZYGOS SYSTEM. MRI...
 shows duplicity of the IVC (red arrow), each side draining the respective common iliac veins, in a path adjacent to the aorta (yellow arrow). The left IVC crosses to the right side just after the confluence of the renal veins through a venous trunk (white arrow), draining shortly afterwards to the single hepatic segment of the IVC (blue arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 14:
DUPLICITY OF THE IVC. MDCT (A to D – axial, E – coronal e F – 3D...
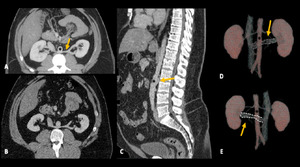
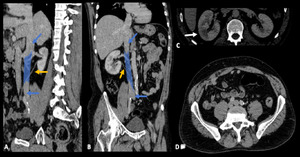
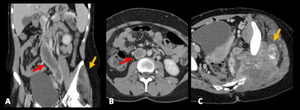
 shows the right ureter (yellow arrow) posterior to the IVC in a 39 years old patient reporting recurrence urinary tract infetion, with right flank pain and fever. Note the signs of ipsilateral pyelonephritis (white arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 15:
RETROCAVAL URETER. MDTC (A – oblique sagittal, B – oblique coronal, C and D...

Fig. 16:
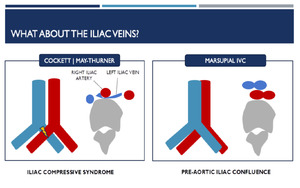
What about THE ILIAC VEINS?
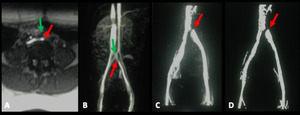
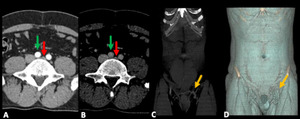
 shows compression of the left common iliac vein (red arrow) between the right common iliac artery (green arrow) and the underlying vertebral body. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 17:
MAY-TURNER SYNDROM | COCKETT. MRI (A – axial T1 post contrast and B to D –...
 shows severe compression of the left common iliac vein (red arrow), with signs of chronic thrombosis, between the right common iliac artery (green arrow) and the underlying vertebral body. Note the development of regional collateral circulation (yellow arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 18:
MAY-TURNER SYNDROM | COCKETT. MDCT (A and B – axial, C – coronal MIP, D –...

Fig. 19:
Another SITUATIONS AND TRAPS WE CAN FIND!
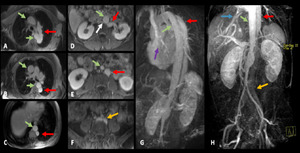
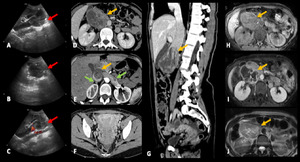
 shows expansive heterogeneous lesion in the suprarenal and renal segments of the IVC , predominantly hypoechoic and without vascularization to the Doppler study (red arrow) in a 42 years old male patient with right flank pain and fever. MDCT in the venous phase (D, G and H) and arterial phase (F); and MRI (I – T1, J – T1 post contrast, K – T2), in axial acquisitions (D to F and I to K) and coronal (G) show mass with heterogenous enhancement, presenting areas of liquefaction / central necrosis (yellow arrow). Note the relation of the lesion with the renal veins (green arrow) and the presence of pelvic varicose veins in F. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 20:
LEIOMYOSARCOMA OF IVC. Ultrasound images (A - C) shows expansive heterogeneous...
 shows right suprarenal carcinoma (yellow arrow) with signs of invasion of the hepatic segment of de IVC (red arrow) determining its thrombosis. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 21:
TUMORAL INVASION OF THE IVC (A to C – axial, D – coronal) shows right...
 with an increase in its diameter and parietal irregularity in a 19 years old female patient with sarcoma in the left thigh (yellow arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 22:
TUMORAL THROMBOSIS OF THE IVC. MDCT shows infrarenal IVC thrombosis (red arrow)...
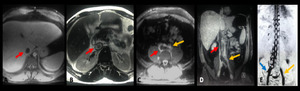
 shows thrombosis of IVC (red arrow) and left common iliac vein (yellow arrow) besides thrombosis of the hepatic and left renal veins (images not included). Note the extensive collateral circulation established through the paravertebral venous plexus from the right common iliac vein (blue arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 23:
THROMBOSIS OF THE IVC. MRI (A – axial T1 venous, B – axial T2, C – axial...
 shows a filter positioned inside the IVC (red arrow). Aorta (yellow arrow) in a 42 years old male patient, with recurrent DVT in lower limbs. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 24:
IVC FILTER. MDCT (A and B - axial, C - coronal MIP, D - sagittal MIP and E - 3D...
 shows membrane (red arrow) in the infrarenal segment of the IVC associated with reduction of local vascular caliber and development of a collateral circulation (B to D). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 25:
OCLUSIVE MEMBRANE IN THE IVC. MRI (A – axial T1 venous, B to D – 3D MIP...
 shows image with fluid signal (red arrow) to the right of the aorta (green arrow) e posterolateral to the right diaphragmatic pillar associated with mild compression of the IVC (yellow arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 26:
CHILI CISTERN. MRI (A – coronal T2, B – axial T2, C – axial T1 venous, D...
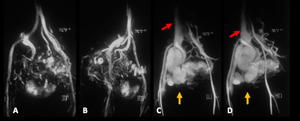
 shows right pelvic arteriovenous fistula with varicose dilatation of the respective iliac vessels (yellow arrow) and IVC (red allow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 27:
PELVIC ARTERIOVENOUS FISTULA. Angioresonance (A and B – early arterial...
 shows the opacification of suprarenal and hepatic segments of the IVC (red arrow) through the mesenteic splenic portal venous system (yellow arrow). Note the usual opacification of the entire IVC in C. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 28:
PORTOCAVAL SHUNT. MRI (A to C – 3D reconstruction) shows the opacification of...
 acquired in the early venous phase, showing the mixture of intravenous contrast through the renal veins (yellow arrow) with uncontrasted blood from the rest of the abdomen and lower limbs. Note the density difference in the IVC (red arrow) before and after the confluence of the renal veins. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 29:
ARTEFATUAL FILLING FAILURE OF THE IVC. MDCT (A – axial, B – coronal e C –...
 shows contrast reflux for the IVC (red arrow) and for the hepatic vens (yellow arrow) in a 43 years old female patient with acute pulmonary thromboembolism. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 30:
RETROGRADE OPACIFICATION OF THE IVC. MDCT (A – axial and B – coronal) shows...