ECR 2019 / C-1662
Role of Magnetic Resonance Imaging (MRI) in assessment of vascular thoracoabdominal emergencies
Congress:
ECR 2019
Poster Number:
C-1662
Type:
Educational Exhibit
Keywords:
Education and training, Computer Applications-3D, MR-Angiography, MR, Vascular, Thorax, Abdomen
Authors:
M. F. P. Pereira, E. C. Raimundo, L. D. P. G. D. Farias, M. D. O. M. Hans, M. D. S. Guedes, P. G. Santana, I. S. Faé, M. V. Galon, I. C. Queiroz; São Paulo/BR
DOI:
10.26044/ecr2019/C-1662
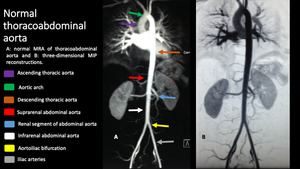
 shows the segments of aorta: ascending (purple arrow), aortic arch (green arrow), descending thoracic (orange arrow), suprarenal (red arrow), renal (blue arrow), infrarenal (white arrow), and aortoiliac bifurcation (yellow arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 1:
Images from a normal Resonance Magnetic Angiography (MRA) shows the segments of...

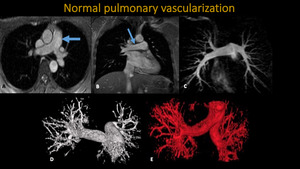
Fig. 2:
MRI and MRA of thorax . A: Axial Trufisp. B: Coronal Trufisp. C:...

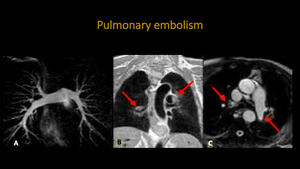
Fig. 3:
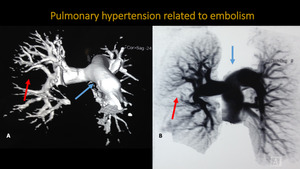
MRI and MRA of thorax. A: MIP 3D demonstrating usual aspect of pulmonary...
, extending to segmental branches (green arrow). Three-dimensional MIP reconstruction points non-opacificated segment of the occluded pulmonary artery (yellow arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
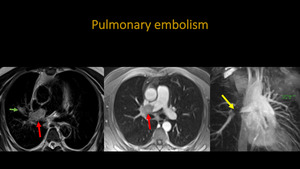
Fig. 4:
Thoracic MRA. A: Axial T2 BLADE. B: Axial T1 post contrast. C: 3D MIP...
. There is also pulmonary trunk ectasia indicating pulmonary hypertension (blue arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
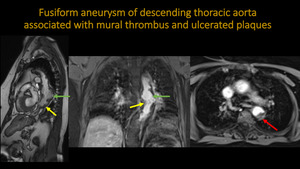
Fig. 5:
Thoracic MRA. A: Three-dimensiona VR reconstruction. B: inverted...
, presenting circular eccentric thrombus (red arrow), and multiple sparse ulcerated plaques (yellow arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
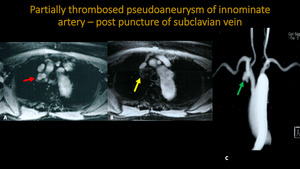
Fig. 6:
MRA of thoracic aorta. A: Sagital TRUFISP. B: Coronal and Axial T1...
, seen partially thrombosed on the yellow arrow. Three-dimensional MIP reconstruction also points the area of pseudoaneurysm (green arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
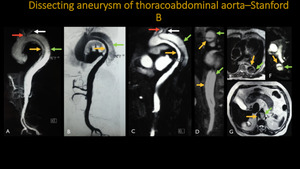
Fig. 7:
MR and MRA of thorax . A and B: Axial T1 post contrast. C: 3D MIP...
, extending to the adrenal segment of the abdominal aorta, dividing the aortic lumens into true (yellow arrow) and false (green arrow). The left subclavian artery (white arrow) originates from the false lumen in the aortic arch.
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 8:
A-D: Three-dimensional MIP reconstructions. E-G: Axial T2. Dissection of the...
.
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 9:
Thoracic aorta MRA. A: 3D FAT-SAT post contrast reconstruction. B: 3D MIP...

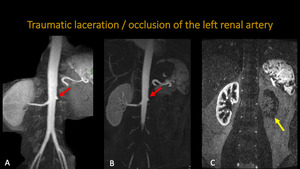
Fig. 10:
MRA of aorta and renal arteries. A and B: 3D MIP reconstructions. C: 3D VR...
. We see also absence of vascularization of the left kidney (yellow arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 11:
Abdominal MRA. A and B: 3D MIP reconstructions. C: Coronal MRA. Patient...

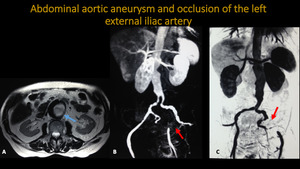
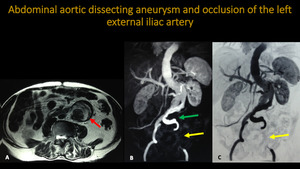
Fig. 12:
Abdominal aortic MRA. A: Axial T2. B and C: 3D MIP reconstructions. Blue arrow:...
. We can see the left common iiac artery being filled by false lumen (green arrow). There is also occlusion of the left external iliac artery (yellow arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
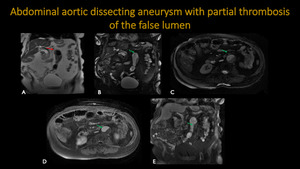
Fig. 13:
Abdominal aortic MRA. A: Axial T2. B and C: 3D MIP reconstructions. Pictures...
 show diffusely ectasiated, tortuous e atheromatous abdominal aorta (red arrow) with infrarrenal aortic aneurysm and partial thrombosis of its lumen (green arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
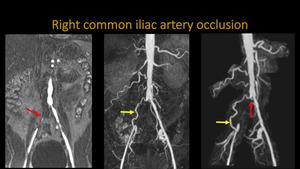
Fig. 14:
MR Images (A – coronal T2, B – coronal FIESTA, C – sagital FIESTA, D –...
. We can see also refilling of the distal segment of right external iliac artery (green arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
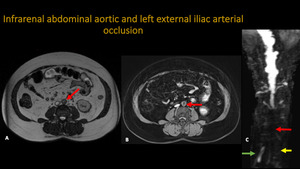
Fig. 15:
MRA. A: Axial T2. B: Axial T1 post-contrast. C: 3D MIP reconstruction. Pictures...
 in the infrarenal segment of the abdominal aorta with bilateral extension to the respective common iliac arteries and exclusion of the partially thrombosed fusiform aneurysm (yellow dotted line), not identified in the angiographic reconstructions post-contrast. Note the usual characterization of the adrenal aortic segment (yellow arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
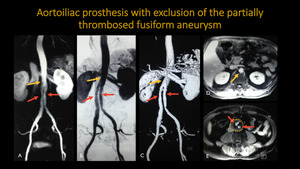
Fig. 16:
Abdominal aortic prosthesis with exclusion of the aneurysm: angioresonance...
, with filling of ipsilateral external and internal iliac arteries by colateral branches (yellow arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
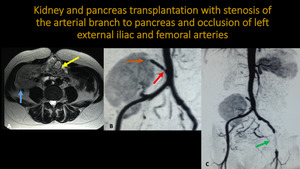
Fig. 17:
Abdominal and thoracic aortic MR angiography. A: Coronal T1 post contrast. B...
 and pancreas (yellow arrow) transplanted in right iliac fossa. There is stenosis of the proximal segment of the arterial branch to pancreas (red arrow) and occlusion of the distal branch (orange arrow). It is still observed occlusion of left external iliac and femoral arteries (green arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
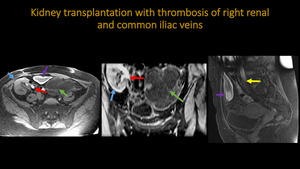
Fig. 18:
Abdominal MR and abdominal aortic MRA. A: Axial T2. B and C: 3D MIP...
, abrupt tapering with occlusion of the right renal and common iliac veins (red and yellow arrows respectively). Additional findings include hemorrhage ovarian cyst (green arrow)) and an adjacent small hemorrhage collection (purple arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
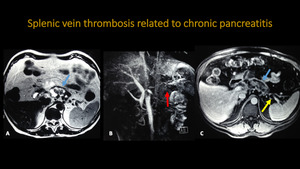
Fig. 19:
Abdominal MR. A: Axial T1 FS. B: Coronal T1 FS. C: Sagital T1 FS. Pictures...
, associated with splenic vein thrombosis (yellow arrow), and no opacification of the vessel on 3D reconstruction (red arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
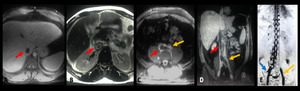
Fig. 20:
Abdominal MR and MRA. A: Axial T2. B: 3D MIP reconstruction. C:. Axial T1 post...
 and left common iliac vein thrombosis (yellow arrow), also hepatic veins and left renal vein thrombosis (images not included). Note the extensive collateral circulation established through the vertebral plexus from the right common iliac vein (blue arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
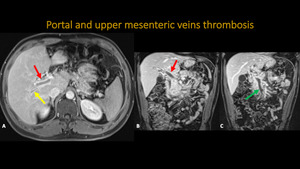
Fig. 21:
Thrombosis of the left common iliac vein and inferior vena cava: angioresonance...
, extending to upper mesenteric vein (green arrow). There is portal parietal thickening with hyperenhancement, inferring inflamatory process/vasculitis.
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
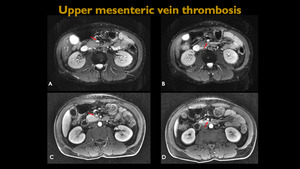
Fig. 22:
Abdominal MR and MRA. A: Axial T1 post contrast. B and C: Coronal T1 post...

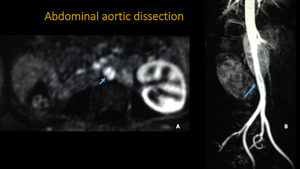
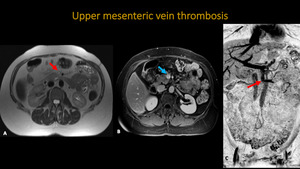
Fig. 23:
Abdominal MR – A and B Axial diffusion. C and D: Axial T1 post-contrast....
 and filling failure inside the vessel (blue arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
Fig. 24:
Abdominal MR and MRA. A: Axial T2. B: Axial T1 post-contrast. C: 3D MIP...