We conduced a review of the literature and a retrospective analyses of reviewed medical records and imaging studies of 28 patients with situs anomalies.
The clinical features and imaging findings will be presented by anatomical sections,
multiplanar recontructons and a pictorial scheme.
Situs solitus with levoversion is the normal anatomic state,
with a trilobed right lung and a bilobed left lung; the morphologic right atrium is to the right of the morphologic left atrium and the cardiac apex is left-sided.
The spleen,
stomach,
and aorta located on the left and the liver and inferior vena cava (IVC) located on the right.
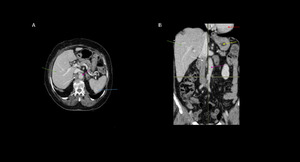
Fig. 1: 70 years old partient. Abdominal CT on axial (A) and coronal (B) demonstrate situs solitus with levoversion (red arrow) and the spleen (blue arrow) , stomach (yellow arrow) , aorta (pink arrow) located on the left and the liver (green arrow) and inferior vena cava (IVC) (white arrow) located on the right side.
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil
Congenital heart disease occurs in less than 1% of individuals with situs solitus
Situs inversus indicates mirror-image location of the viscera relative to situs solitus.
There are two major subcategories of situs inversus: situs inversus with dextrocardia and situs inversus with levocardia.
Situs inversus with dextrocardia is more common and is characterized by mirror- imagelocation of the heart and viscera relative to situs solitus,
with thecardiac apex ,
spleen,
stomach,
and aorta located on the right andthe liver and IVC located on the left.
Congenital heart disease occurs in 3%–5% of cases.
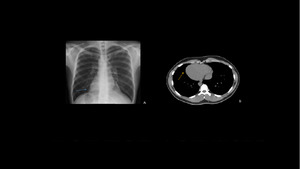
Fig. 2: (A): Chest X-ray showing dextrocardia (black arrow) and a right subphrenic gastric bubble (yellow arrow). (B): Thorax CT image with dextrocardia (yellow arrow).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil
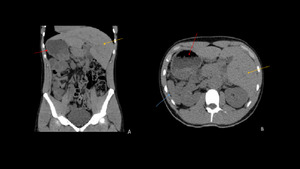
Fig. 3: (A): Coronal CT image showing a left-sided leaver (yellow arrow). (B) axial CT image showing spleen (blue arrow) , stomach (red arrow) , and aorta located on the right.
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil
In contrast,
situs inversus with levocardia is an ex-tremely rare variant that is characterized by mirror-image location of the viscera relative to situs solitus and a left-sided cardiac apex.
Nearly 95% affected individuals have congenital heart.
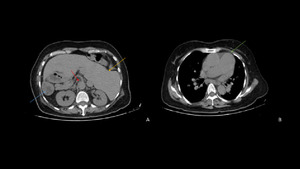
Fig. 4: (A):axial CT image showing liver and IVC on the left (red arrow); spleen (blue arrow) and aorta (red arrow) on the right. (B): Thorax CT image showing the cardiac apex located on the left and a cardiac enlargement .
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil
Twenty percent of patients with situs inversus totalis have Kartagener's syndrome ,
a variant of primary ciliary dyskinesia which is associated with respiratory clinical manifestations due to ciliary dysfunction,
such as chronic bronchitis,
bronchiectasis ,
chronic rhinosinusitis and chronic otitis media.
Male infertility is another relatively common manifestation due to defects in axonemal components in the sperm tail.
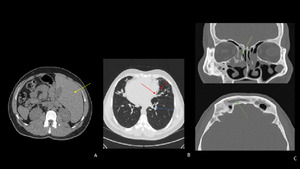
Fig. 5: (A):abdominal CT image showing left-sided liver (yellow arrow). (B): thoracic CT lung-window showing bronchiectasis (red arrow) with thickened bronchial wall (blue arrow) . (C):coronal CT showing mucosal thickening and opacification of paranasal sinuses consistent with sinusitis(green arrows).
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil
Failure of normal lateralization results in abnormal bilateral symmetry of normally asymmetric viscera and duplication of either right- or left-sided structures.
These conditions present withinde terminate situs or situs ambiguous and are often referred to heterotaxy syndromes.
Situs ambiguous is not characterized by a single set of abnormalities but by a spectrum of abnormalities. The two major subcategories of situs ambiguous are situs ambiguous with polysplenia and situs ambiguous with asplenia.
Situs ambiguous with polysplenia is characterized in general by midline or ambiguous location of the majority of the abdominal organs and multiple spleens.
No single anomaly that is pathognomonic for this condition affected patients have a lower prevalence of congenital heart disease (50%– 90%) and less severe defects than do those with situs ambiguous with asplenia .
Although this anomaly has no pathognomonic feature,
a sufficient number of associated findings occur in the majority of patients to allow the diag- nosis to be established.
Abdominal anomalies include multiple small rounded spleens,
a symmetric or transverse liver,
biliary atresia,
and malrotation of the bowel. Abnormalities of systemic venous drainage are common and include interruption of the intrahepatic IVC with azygos continuation,
duplication of the SVC,
and partial anomalous pulmonary venous return.
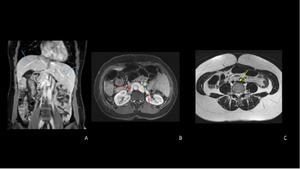
Fig. 6: (A): coronal abdominal MRI showing right and left hepatics veins (blue arrows) draining directly to right atrium. (B): axial MRI showing the absence of inferior vena cava with renal veins (red arrows) draining to azygus system (green arrow) . (c): iliacs veins union (yellow arrow) on the left side of pelvic region.
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil
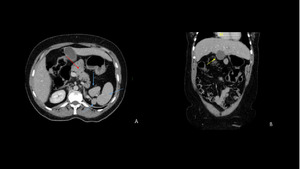
Fig. 7: (A):axial abdominal CT image showing multiples spleens (blue arrows) and abcesnce of the pancrea´s tail and a anular configuration (red arrow).(B): midle-lined gallbladder (yellow arrow) and intestinal malrotation signs.
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil
Heterotaxy with asplenia or Ivemark's syndrome is characterized by an absent spleen and duplication of right-sided structures (bilateral right-sidedness). Bilateral right-sidedness anomalies include bilateral trilobed lungs with eparterial bronchi.
Cardiac anomalies associated with asplenia are usually severe,
are present at an early age,
and have a poor prognosis.
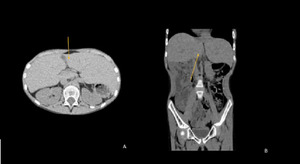
Fig. 8: CT axial and coronal images demonstrate an example of Ivemark's syndrome : middle line liver and asplenia.
References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil

 and coronal (B) demonstrate situs solitus with levoversion (red arrow) and the spleen (blue arrow) , stomach (yellow arrow) , aorta (pink arrow) located on the left and the liver (green arrow) and inferior vena cava (IVC) (white arrow) located on the right side. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
: Chest X-ray showing dextrocardia (black arrow) and a right subphrenic gastric bubble (yellow arrow). (B): Thorax CT image with dextrocardia (yellow arrow). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
: Coronal CT image showing a left-sided leaver (yellow arrow). (B) axial CT image showing spleen (blue arrow) , stomach (red arrow) , and aorta located on the right. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
:axial CT image showing liver and IVC on the left (red arrow); spleen (blue arrow) and aorta (red arrow) on the right. (B): Thorax CT image showing the cardiac apex located on the left and a cardiac enlargement . References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
:abdominal CT image showing left-sided liver (yellow arrow). (B): thoracic CT lung-window showing bronchiectasis (red arrow) with thickened bronchial wall (blue arrow) . (C):coronal CT showing mucosal thickening and opacification of paranasal sinuses consistent with sinusitis(green arrows). References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
: coronal abdominal MRI showing right and left hepatics veins (blue arrows) draining directly to right atrium. (B): axial MRI showing the absence of inferior vena cava with renal veins (red arrows) draining to azygus system (green arrow) . (c): iliacs veins union (yellow arrow) on the left side of pelvic region. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
:axial abdominal CT image showing multiples spleens (blue arrows) and abcesnce of the pancrea´s tail and a anular configuration (red arrow).(B): midle-lined gallbladder (yellow arrow) and intestinal malrotation signs. References: Hospital Alvorada/ Americas Serviços Médicos, São Paulo / Brazil")
