◊Peritoneal tuberculosis
Tuberculosis is still endemic in developing countries.
In the developed world there is some resurgence of the disease caused by immigration,
AIDS and the increased use of immunosuppressant drugs 2.
Peritoneal tuberculosis accounts for 1-3% of cases and it is the 6th most common extra-pulmonary site of tuberculosis 2.
There are three types of peritoneal tuberculosis 2:
- Wet type: abundant ascites and increase density (20-45HU)
- Fixed fibrotic type: peritoneal masses adherent to neighbouring structures; loculated ascites ( Fig. 10 )
- Dry or plastic type: Less common.
Fibrous reaction in the peritoneum; cake-like omentum ( Fig. 9 )
The diagnosis of peritoneal tuberculosis may be difficult.
Some imaging signs can be helpful 2:
- Presence of mesenteric macronodules with or without calcifications
- Splenomegaly and spleen calcifications
- Involvement of ileocecal wall
- Lymphadenopathy (retroperitoneal/peripancreatic) with hypodense centre and ring enhancement.
- Peritoneal thickening is smoother and more regular ( Fig. 10 )
Peritoneal tuberculosis may mimic peritoneal carcinomatosis so histopathological or laboratory confirmation are required before treatment.
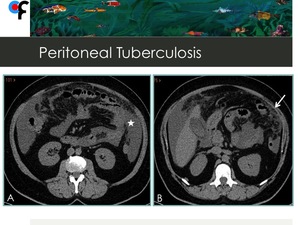
Fig. 9: 56-year-old female patient with vague abdominal symptoms and weight loss. CT showed loculated ascites(star) and thickening of greater omentum (arrow).
References: Department of Radiology, Champalimaud Foundation, Lisbon
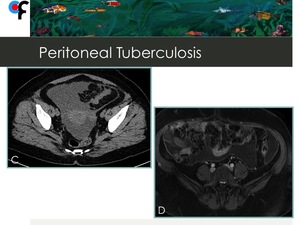
Fig. 10: 56-year-old female patient with vague abdominal symptoms and weight loss. Fig.C- CT showed pelvic loculated ascites; Fig.D- MRI showed enhancement and regular thickening of parietal peritoneum. A gynecological malignancy was suspected but CT and MRI imaging ruled out that hypothesis. The diagnosis was confirmed by a positive TB ascitic fluid culture.
References: Department of Radiology, Champalimaud Foundation, Lisbon
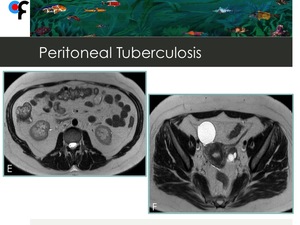
Fig. 11: Peritoneal tuberculosis in a 56-year-old female patient. Fig. E and F correspond to MRI performed after TB treatment. There was a complete regression of all peritoneal findings.
References: Department of Radiology, Champalimaud Foundation, Lisbon
◊Tubo-Ovarian Abscess with Peritonitis
Pelvic inflammatory disease (PID) can be associated with smooth and uniform enhancing peritoneal thickening and pelvic fat haziness.
The intraperitoneal spread of PID can cause perihepatitis.
In women presenting with PID,
perihepatitis and right upper abdominal pain are known as Fitz-Hugh-Curtis syndrome 1.
Tubo-ovarian abscess (TOA) is a serious acute complication of acute pelvic inflammatory disease (30% of patients) 3.
It is a polymicrobial infection typically occurring in young sexually active women,
with a high prevalence of anaerobes -Bacteroides species 3.
Imaging findings :4,5,6
- Thick-walled fluid mass in adnexal location ( Fig. 12 ,
Fig. 13 )
- Septation ( Fig. 13 )
- Thickening and anterior displacement of mesosalpinx/round ligament
- Hydronephrosis
- Infiltration of the omentum and mesentery (Fig. 12 )
- Air within the mass (22-38% of the cases) ( Fig. 14 )
- Tubular or cystic satellite lesions
Differential diagnosis of TOA and ovary malignancy with peritoneal carcinomatosis can be challenging when clinical and lab data are vague and imaging features are atypical.
MRI is the most sensitive and specific imaging technique in the diagnosis of TOA mimicking ovarian cancer 4.
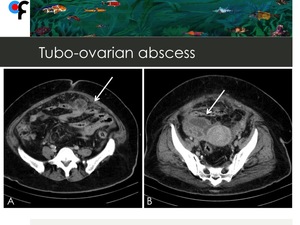
Fig. 12: 51-year old woman presented to the ER with fever and abdominal pain. CT showed infiltration of the omentum and a multiloculated right adnexal mass (arrows). Ovarian cancer with peritoneal carcinomatosis was suspected.
References: Department of Radiology, Champalimaud Foundation, Lisbon
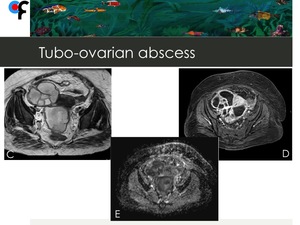
Fig. 13: 51-year-old woman presented to the ER with fever and abdominal pain. MRI showed a multiloculated right adnexal mass with mucin-like signal intensity on T2 WI (Fig.C), marked enhancement on post-contrast images (Fig.D) and low ADC values (Fig.D). Ovarian cancer with peritoneal carcinomatosis was suspected.
References: Department of Radiology, Champalimaud Foundation, Lisbon

Fig. 14: 51-year-old woman presented to the ER with fever and abdominal pain. CT performed 1 week after admission showed the presence of air within the mass and treatment with metronidazole was initiated. After treatment for TOA there was a complete regression of imaging findings.
References: Department of Radiology, Champalimaud Foundation, Lisbon
◊Peritoneal Mesothelioma
Mesotheliomas are rare neoplasms that arise from the mesothelial cells forming the serous membranes of the pleura,
peritoneum,
or pericardium 7.
Peritoneal involvement is reported in 25% of cases 2.
Peritoneal mesothelioma,
as with other forms of mesothelioma,
is related to asbestos exposure,
which is found in 50% of the cases 7.
There are 3 different pathological subtypes of peritoneal mesothelioma 7:
- Malignant mesothelioma ( Fig. 15 )
- Cystic mesothelioma
- Well-differentiated papillary mesothelioma
The clinical and imaging features of peritoneal mesotheliomas vary among these subtypes.
Macroscopic features of peritoneal mesothelioma are similar to those seen in peritoneal carcinomatosis:
- Ascites
- Diffuse and/or nodular thickening of the peritoneal serous membrane
- Invasion of the greater omentum: omental cake/ mesenteric masses with or without calcifications.
( Fig. 15 A)
The diagnosis requires pathological assessment.
However,
some features are more suggestive of peritoneal mesothelioma:
- Occupational exposure to asbestos
- Concurrent pleural involvement ( Fig. 15 B)
- Absence of lymphadenopathy or spread to distant organs
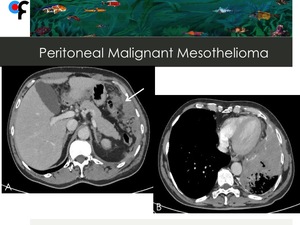
Fig. 15: Malignant Mesothelioma at a 57-year-old male patient. Fig.A shows invasion of the greater omentum (arrow). Fig.B shows concurrent left pleural involvement. Lymphadenopathy or spread to distant organs were absent. The patient is a medical doctor with no past history of occupational exposure to asbestos.
References: Department of Radiology, Champalimaud Foundation, Lisbon
◊Peritoneal Deciduosis
Decidualization corresponds to the process occurring in pregnancy where the endometrium undergoes specialized transformation to support the growing fetus.
It appears to be related to a hormonal response to progesterone 8.
Deciduosis is defined as the presence of decidual tissue in an ectopic location and usually occurs in the context of a diagnosed endometriosis.
It occurs in the pelvis,
most commonly in the ovaries,
the anterior and posterior surfaces of the uterus,
fallopian tubes,
but also in the peritoneum,
omentum ( Fig. 16 ),
pleura and bladder 8.
Although it is a benign condition typically asymptomatic and incidentally found,
there are reported cases of pain and intraperitoneal haemorrhage.
Its occurrence in non-pregnant women is rare and this diagnosis should trigger an active search for a source of hormone production such as exogenous administration of progesterone or a hormone producing tumor.
Ectopic deciduosis can mimic a malignant tumor,
particularly in patients with no previous history of endometriosis that present with peritoneal deciduosis
( Fig. 16 ,
Fig. 18 ).
The diagnostic dilemma is to differentiate between benign decidualized tissue that can be managed conservatively from peritoneal carcinomatosis 8.
It is very difficult to differentiate one from another based on imaging findings,
however,
the radiologist should be aware of this entity.
The final diagnosis is histopathological ( Fig. 19 ).

Fig. 16: 40-year-old female patient presented to the ER with symptoms of urinary tract infection. Abdominal and pelvic CT showed diffuse omental fat stranding in the upper and lower abdomen.
References: Department of Radiology, Champalimaud Foundation, Lisbon
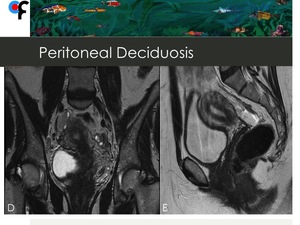
Fig. 17: 40-year-old female patient presented to the ER with symptoms of urinary tract infection. Abdominal and pelvic CT showed diffuse omental fat stranding in the upper and lower abdomen. Pelvic MRI was performed to exclude gynecologic malignancy and didn't show abnormal findings.
References: Department of Radiology, Champalimaud Foundation, Lisbon
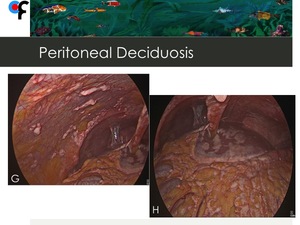
Fig. 18: 40-year-old female patient presented to the ER with symptoms of urinary tract infection. Abdominal and pelvic CT showed diffuse omental fat stranding in the upper and lower abdomen. Pelvic MRI was performed to exclude gynecologic malignancy and didn't show abnormal findings. At diagnostic laparascopy, multiple and confluent nodules were seen in the mesentery and in the small bowell serosa. The macroscopic aspect was concordant with peritoneal carcinomatosis and the laparascopic peritoneal cancer index (PCI) was: 39/39.
References: Champalimaud Foundation, Lisbon
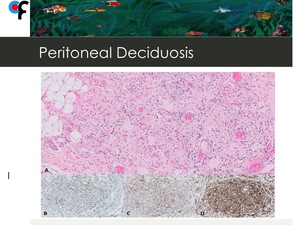
Fig. 19: 40-year-old female patient presented to the ER with symptoms of urinary tract infection. Abdominal and pelvic CT showed diffuse omental fat stranding in the upper and lower abdomen. Pelvic MRI was performed to exclude gynecologic malignancy and didn't show abnormal findings. At diagnostic laparascopy, multiple and confluent nodules were seen in the mesentery and in the small bowell serosa. The macroscopic aspect was concordant with peritoneal carcinomatosis and the laparascopic peritoneal cancer index (PCI) was: 39/39.
Histology of the biopsies performed at diagnostic laparascopy was concordant with peritoneal deciduosis. The patient wasn't pregnant and denied history of pregnancy or abortion.
A- H&E stain. Infiltration of adipocytes by nodular infiltrates of large cells with eosinophilic cytoplasm, small and eccentric nuclei, associated with mild chronic inflammatory infiltrates and vascular congestion. B, C and D- Immunohistochemical stains showing the decidual cells to be positive for progesterone receptors(B), desmin(C) and vimentin (D).
References: Department of Pathology, Champalimaud Foundation, Lisbon. Courtesy of Dr. Vanessa Henriques
◊Pseudomyxoma Peritonei
Pseudomyxoma peritonei is an uncommon borderline malignancy characterized by the presence of mucin-secreting cells on peritoneal surfaces 10.
The primary tumour is thought to originate in the appendix in men.
In women,
synchronous ovarian and appendiceal disease is common and immuno-histochemistry and molecular genetic studies support the theory that the ovarian tumour is metastatic from a perforated appendiceal mucinous tumour10.
CT is the optimal imaging technique for diagnosis and staging of this entity.
Imaging findings: 2,10
- Peritoneal nodules
- Scalloping of visceral surfaces (liver and spleen)
- Visualization of fluid or a soft tissue mass on the appendix ( Fig. 20 )
- Mucinous ascites (in contrast to fluid ascites) ( Fig. 21 )
- Curvilinear calcifications
- Characteristic pattern of distribution:
-At first the disease is limites at sites with peritoneal attachments: ileocaecal region, ligament of Treitz, sigmoid colon
-Relative sparing of small bowel and its mesentery
-Compartmentalization in the central abdomen (greater omentum and diaphragmatic peritoneum)
Once these patients have prolonged survival if an aggressive surgical approach is taken,
it is very important to establish this diagnosis and to predict the likelihood of complete cytoreduction by imaging 2.
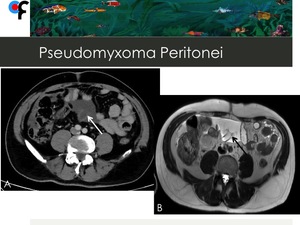
Fig. 20: 67-year-old male patient with history of prostate adenocarcinoma. A,B- A tubular cystic mass with thin and enhancing walls, which was contiguous with the base of the cecum was detected (arrows). An appendiceal mucocele was suspected. C,D- Abdominal and pelvic ascites. Presence of hypointense foci within the ascites (arrow).
At surgery, mucinous ascites and a ruptured appendiceal tumor were detected. Final diagnosis was compatible with pseudomyxoma peritonei.
References: Department of Radiology, Champalimaud Foundation, Lisbon
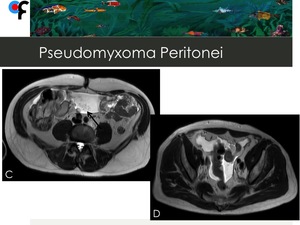
Fig. 21: 67-year-old male patient with history of prostate adenocarcinoma. A,B- A tubular cystic mass with thin and enhancing walls, which was contiguous with the base of the cecum was detected (arrows). An appendiceal mucocele was suspected. C,D- Abdominal and pelvic ascites. Presence of hypointense foci within the ascites (arrow).
At surgery, mucinous ascites and a ruptured appendiceal tumor were detected. Final diagnosis was compatible with pseudomyxoma peritonei.
References: Department of Radiology, Champalimaud Foundation, Lisbon
◊Disseminated Peritoneal Leiomyomatosis
Disseminated peritoneal leiomyomatosis (DPL) is a rare benign disorder of unknown origin that is characterized by the presence of leiomyomas growing along the submesothelial tissues of the abdominopelvic peritoneum 11.
It is associated with hormonal factors such as pregnancy,
long-term use of oral contraceptives and occasionally,
granulosa cell tumors of the ovary 11.
This entity usually has good prognosis,
with regression of the leiomyomas after childbirth or after removal of the hormonal production source.
However,
cases of recurrence at a later stage and sarcomatous transformation have been reported 2.
Imaging findings: 2,11
- Multiple solid subcentimetric peritoneal nodules with variable enhancement patterns similarly to uterine leiomyomas ( Fig. 22 )
- Large soft-tissue peritoneal masses
- The lesions are more commonly located in the pelvic peritoneum and greater omentum but can also be found in the uterus,
ovaries and on the visceral side of the intestinal peritoneum.
The most important entity in the differential diagnosis of DPL is peritoneal carcinomatosis.
The absence of clinical symptoms and the absence of ascites,
lymphadenopathies and liver metastases at imaging in these patients should alert the radiologist towards an alternative diagnosis to peritoneal carcinomatosis.
Exploratory laparotomy and surgical biopsies are often required for a definitive diagnosis of DPL however,
the results of an imaging-guided percutaneous biopsy may be suggestive or indicative of the diagnosis 11.
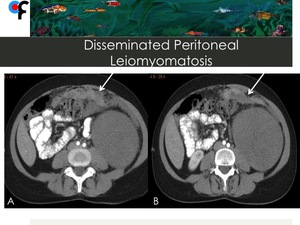
Fig. 22: 46-year-old female patient with no clinical symptoms and history of uterine leiomyomas. Abdominal and pelvic CT was performed to clarify an incidental left kidney lesion detected at ultrasound. A,B- CT showed multiple confluent nodules with different densities infiltrating the greater omentum and resembling omental cake. C,D- A large soft tissue mass was detected at left kidney. Pelvic CT demonstrated the presence of multiple uterine leiomyomas. The nodules located in the greater omentum and the left kidney mass were submitted to CT-guided percutaneous biopsy. The results of the greater omentum nodules biopsy were compatible with disseminated peritoneal leiomyomatosis. The results of the left kidney mass were compatible with tubular mucinous and spindle cell tumor.
References: Department of Radiology, Champalimaud Foundation, Lisbon
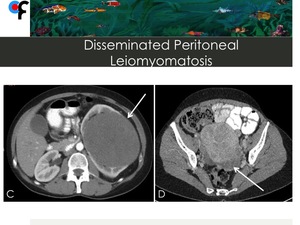
Fig. 23: 46-year-old female patient with no clinical symptoms and history of uterine leiomyomas. Abdominal and pelvic CT was performed to clarify an incidental left kidney lesion detected at ultrasound. A,B- CT showed multiple confluent nodules of different densities infiltrating the greater omentum and resembling omental cake. C,D- A large soft tissue mass was detected at left kidney. Pelvic CT demonstrated the presence of multiple uterine leiomyomas. The nodules located in the greater omentum and the left kidney mass were submitted to CT-guided percutaneous biopsy. The results of the greater omentum nodules biopsy were compatible with disseminated peritoneal leiomyomatosis. The results of the left kidney mass were compatible with tubular mucinous and spindle cell tumor.
References: Department of Radiology, Champalimaud Foundation, Lisbon
◊Peritonitis secondary to Acute Abdominal Inflammatory Conditions
Acute abdominal inflammatory conditions may be responsible for peritonitis,
usually localized.
This type of peritonitis is characterized by 1:
- Small sized fluid-like collections surrounding the involved gastrointestinal segment ( Fig. 25 )
- Smoothly thickened and enhancing peritoneum
- Increased density within the adjacent mesentery ( Fig. 24)
Nodular peritoneal thickening is the hallmark of peritonitis induced by inflammatory conditions in patients with primary or metastatic neoplastic GI involvement 1.
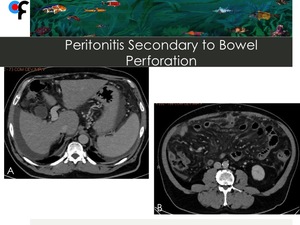
Fig. 24: 56-year-old male patient presented to the ER with abdominal pain. Lab work showed mild leukocytosis. An abdominal and pelvic CT was performed. A,B- CT showed ascites, diffuse stranding of the greater omentum and increased density of the mesentery. A peritoneal carcinomatosis was initially suspected.
C,D- Axial and sagittal CT showing the presence of a small and wall-thickened fluid collection with an intra-lesional linear calcification, located anteriorly to the transverse colon.
The patient underwent surgery and a peritonitis secondary to a perforation of the transverse colon caused by a fish bone was detected.
References: Department of Radiology, Champalimaud Foundation, Lisbon
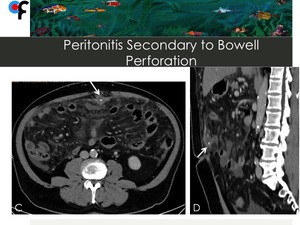
Fig. 25: 56-year-old male patient presented to the ER with abdominal pain. Lab work showed mild leukocytosis. An abdominal and pelvic CT was performed. A,B- CT showed ascites, diffuse stranding of the greater omentum and increased density of the mesentery. A peritoneal carcinomatosis was initially suspected.
C,D- Axial and sagittal CT showing the presence of a small and wall-thickened fluid collection with an intra-lesional linear calcification, located anteriorly to the transverse colon (arrows).
The patient underwent surgery and a peritonitis secondary to a perforation of the transverse colon caused by a fish bone was detected.
References: Department of Radiology, Champalimaud Foundation, Lisbon

 and thickening of greater omentum (arrow). References: Department of Radiology, Champalimaud Foundation, Lisbon")


. Ovarian cancer with peritoneal carcinomatosis was suspected.
References: Department of Radiology, Champalimaud Foundation, Lisbon")
, marked enhancement on post-contrast images (Fig.D) and low ADC values (Fig.D). Ovarian cancer with peritoneal carcinomatosis was suspected.
References: Department of Radiology, Champalimaud Foundation, Lisbon")

. Fig.B shows concurrent left pleural involvement. Lymphadenopathy or spread to distant organs were absent. The patient is a medical doctor with no past history of occupational exposure to asbestos. References: Department of Radiology, Champalimaud Foundation, Lisbon")


 was: 39/39. References: Champalimaud Foundation, Lisbon")
 was: 39/39.
Histology of the biopsies performed at diagnostic laparascopy was concordant with peritoneal deciduosis. The patient wasn't pregnant and denied history of pregnancy or abortion.
A- H&E stain. Infiltration of adipocytes by nodular infiltrates of large cells with eosinophilic cytoplasm, small and eccentric nuclei, associated with mild chronic inflammatory infiltrates and vascular congestion. B, C and D- Immunohistochemical stains showing the decidual cells to be positive for progesterone receptors(B), desmin(C) and vimentin (D). References: Department of Pathology, Champalimaud Foundation, Lisbon. Courtesy of Dr. Vanessa Henriques")
. An appendiceal mucocele was suspected. C,D- Abdominal and pelvic ascites. Presence of hypointense foci within the ascites (arrow).
At surgery, mucinous ascites and a ruptured appendiceal tumor were detected. Final diagnosis was compatible with pseudomyxoma peritonei. References: Department of Radiology, Champalimaud Foundation, Lisbon")
. An appendiceal mucocele was suspected. C,D- Abdominal and pelvic ascites. Presence of hypointense foci within the ascites (arrow).
At surgery, mucinous ascites and a ruptured appendiceal tumor were detected. Final diagnosis was compatible with pseudomyxoma peritonei. References: Department of Radiology, Champalimaud Foundation, Lisbon")



.
The patient underwent surgery and a peritonitis secondary to a perforation of the transverse colon caused by a fish bone was detected. References: Department of Radiology, Champalimaud Foundation, Lisbon")