Obstetric ultrasound is the modality of choice for fetal assessment,
is essential in the diagnosis and classification of abdominal wall defects,
it’s wide and common use has increased the prenatal detection of these abnormalities.
To this date,
most of the AWDs are being detected as soon as 11th – 14th week of pregnancy,
and it has been described that by the 12th week we should be able to detect all cases of omphalocele and gastroschisis.
Sonographic approach
Before we begin the exploration we have to mention that,
when evaluating the abdominal wall the anterior aspect is better demonstrated in axial planes,
where it is delineated in its outer surface by amniotic fluid.
The first step is to measure the abdominal circumference,
this has to be done according to the International Society of Ultrasound in Obstetrics & Gynecology (ISUOG) guidelines,
getting an image in the axial plane of the abdomen,
observing the umbilical vein at the level of the portal sinus and the gastric bubble,
the kidneys should not be visible.
Fig. 1
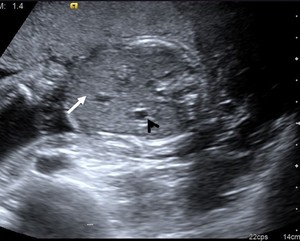
Fig. 1: Abdominal circumference following the ISUOG guidelines. Axial image of the abdomen showing the stomach bubble (arrowhead) as well as the portal sinus (arrow). The kidneys are not visible.
References: Imaging Department, Hospital Ángeles Lomas. Estado de México.
In cases of AWDs,
evaluating cord insertion is critical.
In general terms,
if the anterior abdominal wall,
cord insertion,
and bladder are evaluated and normal,
most of the defects can be ruled out.
Evaluating the anterior abdominal wall beneath the cord insertion can result difficult in case of lower limbs flexion,
a midline sagittal plane can result helpful in this setting.
Fig. 2

Fig. 2: Sagittal plane of a fetus with omphalocele, showing the cord with herniated bowel at its insertion.
References: Maternal Fetal Medicine Clinic, Hospital Ángeles Lomas. Estado de México.
We can divide the abdominal wall defects in terms of its cord insertion,
weather is normal or abnormal.
1.
Defects with normal cord insertion:
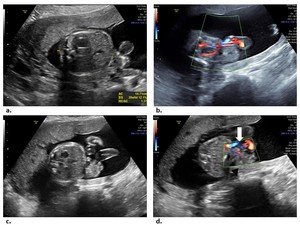
Fig. 3: Gastroschisis. (a) Axial image shows a small abdominal circumference secondary to herniated bowel. (b) Normal bladder surrounded by umbilical arteries. (c) and (d) show paramedian defect with extruded bowel loops (arrowhead) adjacent to a normal cord insertion (arrow).
References: Maternal Fetal Medicine Clinic, Hospital Ángeles Lomas. Estado de México.
-
Bladder exstrophy: Normal cord insertion,
with persistently “absent” urinary bladder,
a hallmark of this pathology.
The bladder is open to the abdominal wall,
releasing urine to the amniotic cavity,
never visible as a fluid-filled structure.
No bowel herniation is seen.
2.
Defects with abnormal cord insertion:
-
Omphalocele: Herniation of abdominal viscera through an enlarged umbilical ring,
covered by an inner membrane of peritoneum and an outer membrane of amnion,
the umbilical cord inserts on the apex of the herniated sac.
Fig. 4
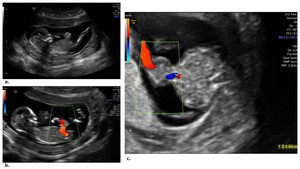
Fig. 4: Omphalocele. (a) and (b) show a sagittal plane where an abnormal cord insertion is seen, there are herniated bowel loops. (c) Axial plane demonstrates herniation of small bowel through a midline defect covered by a membrane, the umbilical cord inserts on the apex of the abdominal wall defect.
References: Maternal Fetal Medicine Clinic, Hospital Ángeles Lomas. Estado de México.
-
Cloacal exstrophy: Omphalocele with an abdominal defect that extends inferiorly,
accompanied by bladder exstrophy (“absent” bladder) and bowel herniation between the bladder halves,
giving the “elephant trunk” appearance.
-
Pentalogy of Cantrell: The full spectrum consists of defects in the lower sternum,
anterior diaphragm,
diaphragmatic pericardium,
and a supraumbilical abdominal wall defect,
usually omphalocele.
This is the most likely diagnosis when omphalocele is associated with ectopia cordis.
Fig. 5

Fig. 5: Pentalogy of Cantrell. (a) Axial image shows a ventral defect with extruding bowel loops (arrowhead). (b) 3D ultrasound demonstrates the fetus with protrusion of the intestinal content (black arrow). (c) and (d) Axial image of the thorax, showing the heart outside the chest, corresponding with ectopia cordis (arrow).
References: Imaging Department, Hospital Ángeles Lomas. Estado de México.
-
Body stalk anomaly: Attachment of visceral organs to the placenta due to a large ventral wall defect and a short or absent umbilical cord. The fetus is in a fixed position with the evisceration of the abdominal content,
wich is adherent to the placental surface without a defined anatomical distribution.

Fig. 6: Abdominoschisis due to amniotic bands. (a) Grayscale ultrasound shows a fetus with undefinable anatomic parts in a fixed position, the umbilical cord is seen (arrow). (a) and (b) Grayscale ultrasound image shows amniotic bands as linear echogenic structures (arrowheads).
References: Imaging Department, Hospital Ángeles Lomas. Estado de México.
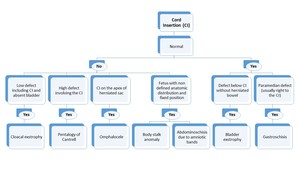
Fig. 7: Algorithmic approach of abdominal wall defects.
References: Modified from Pakdaman, R., Woodward, P.J., Kennedy, A. (2015). Complex Abdominal Wall Defects: Appearances at Prenatal Imaging. RadioGraphics. 35: 636-649.
Key points:
-
We have to remember that physiologic gut herniation is a normal event,
but resolves by the 12th week of gestation,
therefore a diagnosis before this period is impossible.
In case of uncertainty,
a follow up can be made by the 14th week of gestation.
-
Fixed fetal position and non-defined anatomic distribution are the hallmarks of abdominoschisis due to amniotic bands and body stalk anomaly,
however,
in the latter,
the umbilical cord is not seen floating in the amniotic fluid.
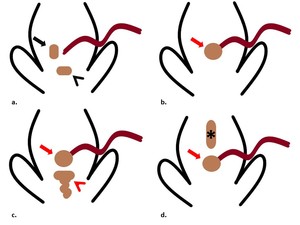
Fig. 8: Graphic illustration of AWDs.
Defects with normal cord insertion: (a), shows a paramedian defect (black arrow) corresponding to gastroschisis. A defect involving the bladder (black arrowhead), without bowel extrusion, corresponds to bladder exstrophy. Defects with abnormal cord insertion: Omphalocele (b), demonstrates herniation of bowel loops trough the umbilical cord insertion (red arrow). (c) Shows a defect with caudal extension and involvement of the bladder, as well as extrusion of bowel loops (red arrowhead), consistent with cloacal exstrophy. (d) Shows a defect with cranial extension (asterisk), corresponding with pentalogy of Cantrell. Both of them (c) and (d) are accompanied by a defect at the cord insertion (red arrow).
References: Imaging Department, Hospital Ángeles Lomas. Estado de México.

 as well as the portal sinus (arrow). The kidneys are not visible. References: Imaging Department, Hospital Ángeles Lomas. Estado de México.")

 Axial image shows a small abdominal circumference secondary to herniated bowel. (b) Normal bladder surrounded by umbilical arteries. (c) and (d) show paramedian defect with extruded bowel loops (arrowhead) adjacent to a normal cord insertion (arrow). References: Maternal Fetal Medicine Clinic, Hospital Ángeles Lomas. Estado de México.")
 and (b) show a sagittal plane where an abnormal cord insertion is seen, there are herniated bowel loops. (c) Axial plane demonstrates herniation of small bowel through a midline defect covered by a membrane, the umbilical cord inserts on the apex of the abdominal wall defect. References: Maternal Fetal Medicine Clinic, Hospital Ángeles Lomas. Estado de México.")
 Axial image shows a ventral defect with extruding bowel loops (arrowhead). (b) 3D ultrasound demonstrates the fetus with protrusion of the intestinal content (black arrow). (c) and (d) Axial image of the thorax, showing the heart outside the chest, corresponding with ectopia cordis (arrow). References: Imaging Department, Hospital Ángeles Lomas. Estado de México.")
 Grayscale ultrasound shows a fetus with undefinable anatomic parts in a fixed position, the umbilical cord is seen (arrow). (a) and (b) Grayscale ultrasound image shows amniotic bands as linear echogenic structures (arrowheads). References: Imaging Department, Hospital Ángeles Lomas. Estado de México.")
. Complex Abdominal Wall Defects: Appearances at Prenatal Imaging. RadioGraphics. 35: 636-649.")
, shows a paramedian defect (black arrow) corresponding to gastroschisis. A defect involving the bladder (black arrowhead), without bowel extrusion, corresponds to bladder exstrophy. Defects with abnormal cord insertion: Omphalocele (b), demonstrates herniation of bowel loops trough the umbilical cord insertion (red arrow). (c) Shows a defect with caudal extension and involvement of the bladder, as well as extrusion of bowel loops (red arrowhead), consistent with cloacal exstrophy. (d) Shows a defect with cranial extension (asterisk), corresponding with pentalogy of Cantrell. Both of them (c) and (d) are accompanied by a defect at the cord insertion (red arrow). References: Imaging Department, Hospital Ángeles Lomas. Estado de México.")