An adequate preoperative evaluation of the patient,
and knowledge of the good prognosis criteria of fistulas,
allow the optimal choice of arteries and veins,
that will be part of the fistula and that will lead to successful access.
Likewise,
the postoperative evaluation that allows to identify the maturity of the arteriovenous fistulas and the associated complications result in an appropriate and functional vascular access over time.
The first choice access is autologous arteriovenous fistula because of its better functioning and long-term duration.
Autologous fistulas have lower morbidity,
mortality and cost compared with grafts and the central venous catheter.
When evaluating the fistulas it is necessary to observe and analyze seven important exploration points such as:
1- Inflow or afferent artery
2- Anastomotic arterial cape.
3- Fistulous path
4- Venous anastomotic cape
5- Outflow or efferent vein.
6- Distal arteries.
7- Proximal veins.
INFLOW study (afferent artery that nourishes the fistula).
The expected spectral morphology is usually low resistance and high speeds.
The maximum systolic velocity is between 100-400cm/s,
taking into account that they are not taken as absolute values to quantify the stenosis.
The diastolic velocity should be between 40-60 cm/s.
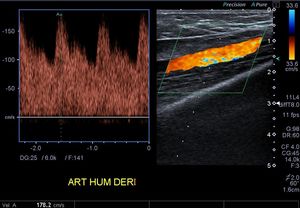
Fig. 3: Spectral analysis of the humeral artery of a patiente with an arterio venous fistula at the elbow. Low resistance and high velocities are observed.
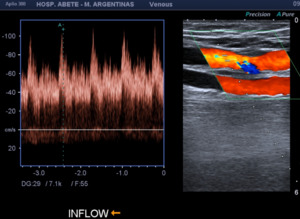
Fig. 4: Inflow (afferent artery that nourishes the fistula). The humeral artery is observed with a spectrum of low resistance and high velocities. VPS: 100 cm/s
ANASTOMOTIC POINTS: The arterial and venous anastomotic points are important sites to review since they can present significant stenosis that compromise the flow of the fistula.
Sometimes a scar retraction or septum can reduce light and compromise flow.
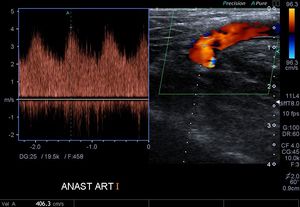
Fig. 5: AV fistula. Arterial anastomotic point.
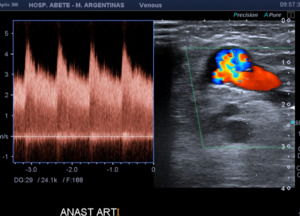
Fig. 6: Arterial anastomosis of an autologous AV fistula. Aliasing is observed, which shows high velocities at that level.
FISTULOUS PATH:
It can be performed with the patient's autologous vein (mostly used) or with prosthetic material.
If it is the first option,
the path of the fistula is usually short.
In the fistulous trajectory,
flow of high speeds will be observed,
with aliasing color and turbulence,
very increased maximum speeds.
A thrill is palpable at the level of the fistula and vein of immediate drainage.
The presence of this thrill will guide us towards the proper functioning of the fistula.
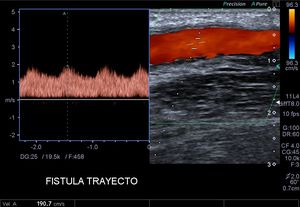
Fig. 7: Arteriovenous fistula path.
Fig. 8: Septum or scar fibrotic septum in the arterial anastomosis, which produces a stenosis of the lumen of the fistula and compromises the functioning of it. Turbulent flow color Doppler is observed inside the fistulous tract, "aliasing"

Fig. 9: Arterio venous prosthetic fistula in the thigh, in a loop form, patent. The double wall observed in the prosthetic material is observed. The light presents aliasing demonstrating high speeds. There is also an organized collection around the arterial anastomotic end.
Fig. 10: Fistulous tract color Doppler with initial arterial flow with high velocity spectrum was observed, with a subsequent venous flow at the venous cape with decreasing velocities. This abrupt change in velocities is a sign of stenosis.
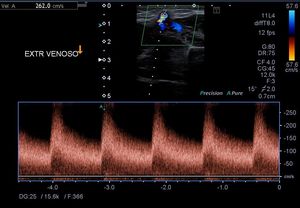
Fig. 11: AV fistula. Venous anastomotic point.
OUTFLOW study: efferent vein draining fistula
The efferent vein is arterialized,
so it is possible to evaluate the spectral morphology and measure velocities.
Normal expected spectral morphology is arterialization or venous pulsatility with low resistance (same as in the artery).
The respiratory changes are conserved.
The systolic velocities are high.
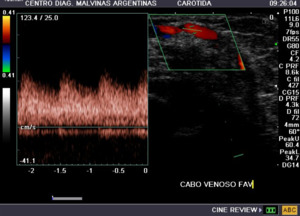
Fig. 12: Venous end of AVF.
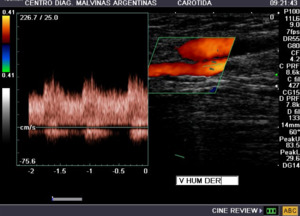
Fig. 13: Arterio venous fistula, humeral drainage vein with presence of pulsatile flow is observed.
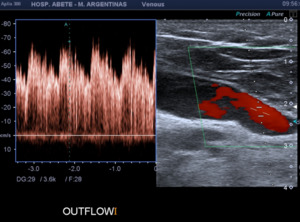
Fig. 14: OUTFLOW. Efferent humeral drainage vein with presence of pulsatile flow is observed. VPS: 70cm/s. Spectrum that for a vein has high speed and low resistance.
Types of arteriovenous fistulas.
Depending on the type of material used,
they are divided into:
Autologous: It is that fistula created from a native vein that is mobilized and anastomosed to a native artery,
presents fewer morbidities than prosthetic ones,
which is why they are the method of choice.
They are usually formed between the radial artery and a superficial vein,
and are named according to the veins and arteries that compose it.
Prosthetic: It is that fistula formed by a prosthetic duct that connects an afferent artery and an efferent vein.
The most frequent anatomical locations are the straight Radio-basilica and the Humero-basilica in loop or "loop",
to the visualization by ultrasound is observed in B-mode,
two parallel echogenic lines.

Fig. 15: Heterologous AV Fistula. The prosthetic material is observed with a double echoic line on its wall that allows to differentiate it from autologous fistulas.
Fig. 16: Twin view images. On the right side, a video is observed in mode B where the prosthetic material of the fistula can be seen which walls present a double echogenic line.
On the left side, the same image but with Colod Doppler with aliasing inside.
The arterial and vein anastomosis show decreased caliber and increased speeds compatible with stenosis sites that should be explored with spectral Doppler to measure velocities.
According to the type of anatomy:
- Lateral-lateral anastomosis
- Lateral-terminal anastomosis (Brescia Cimino)
- End-to-side anastomosis
- Terminal-terminal anastomosis.
Preoperative evaluation for an arteriovenous fistula.
The method of choice to perform the initial exploration of the AVF is the color Doppler ultrasound because it is an easy access method,
low cost and non-invasive,
then we will detail the presurgical evaluation by this diagnostic method.
The preoperative mapping of the arterial and venous territory of the patient who underwent an AV fistula,
increases the rate of autologous AV and thus a higher survival rate in the fistulas.
Doppler evaluation should be performed with a linear transducer of 7.0 MHz or greater.
The patient should be studied in a supine or seated position,
with the arm hanging in order to cause venodilation.

Fig. 17: Patient in supine decubitus, with extended arm, allowing the correct valuation of the AVF.
Table 1: Clinical criteria for the realization of an arteriovenous fistula in the wrist.
Both the arterial system and the superficial and deep venous system of both arms must be evaluated,
from the wrist to the subclavian artery or reverse,
examining direction of flow,
velocities,
spectrum morphology,
presence of thrombosis or occlusions and anatomical variants in both vascular systems.
Arterial and vein calibers must be measured.
The equipment should be adjusted so that we detect slow flows,
by decreasing PRF and increasing the color gain.
The morphological exploration will be done in transverse mode and longitudinal dynamics. The normal anatomy and its variants must be recognized.
The arteries must measure 2 mm or more.
The state of the arterial walls,
calcifications,
thickening,
stenosis and atherosclerosis that usually affects the subclavian and axillary must be confirmed,
but in the diabetic population it can also affect more distal arteries.
The veins should measure 2.5 mm or more and be compressible,
without thrombosis or septa.
The most frequent sites of venipuncture should be thoroughly explored.
It is very important to measure the venous diameter,
place a tourniquet that will generate vasodilatation of the venous tree,
and we must ensure the permeability of the proximal deep veins (brachial,
axillary and subclavian).
Assessing the next venous system is vital,
such as occlusion or obstruction by post-thrombotic chronic changes of the subclavian vein or axillary are common in patients with central catheter placement.
The stenosis of the proximal venous system causes immediate failure of vascular access.
Evaluation of the proximal venous system. Signs of obstruction:
- Vein with difficulty for compression or incompressible.
- Absence of flow to color Doppler.
- Continuous flow instead of phasic with respiratory movements.
Table 2: Non-invasive criteria for the selection of target vessels in the realization of a vascular access for hemodialysis.
Postoperative evaluation.
Doppler is the method of choice to assess the maturity of vascular access.
Measurements are made at a day,
15 days,
and a month later or until a proper diameter and flow of the fistula are observed.
A fistula is considered mature upon evaluation with color Doppler when: the afferent artery becomes low resistance and with high velocities,
the fistula must have a high flow and thrill,
and the efferent vein must dilate and its pattern should become pulsatile and normal.
When presenting VPS 150 at 300 cm/s and VFD 60 at 200 cm/s.
They are indicators of functioning or mature fistula:
- Presence of thrill.
- Venous diameter ˃ 4mm
- Minute volume> 500ml/min.
An AVF is considered clinically mature when it is dilated,
palpable and capable of performing hemodialysis at a flow rate of 350 ml/min in 6 dialysis sessions in 1 month.
Analysis of the flow volume in the fistula.
The calculation of the volume is important to evaluate the dysfunction of access in fistula and grafts.
The volume of flow in the drainage vein can be measured but it is recommended to perform it in the alimentary artery two centimeters before the anastomosis and after the anastomosis,
on the same artery, the calculation of the flow volume in the drainage vein is not recommended because there may be variations in the diameter of the vessel,
dolichoectasia and vibrations that generate turbulence due to the superficial location of the vessel and may alter the result.
It should be done with a large volume of sample,
in a middle place of the fistula or where there is normal flow,
trace the spectrum of 3 to 4 cardiac cycles and measure average speed with a wave plot to measure the volume the formula is used: Flow Volume = Average speed x area x 60.
Complications
- Stenosis
The stenosis occurs in the anastomosis,
or in the drainage vein,
caused by an intimal and fibromuscular hyperplasia generated by the friction of the blood flow in the areas of decreased caliber.
When color Doppler ultrasound are identified as aliasing artifacts.
To perform the calculation of the stenosis,
the cross-sectional area of the stenosis site is measured compared to the transverse area of a normal segment close to the stenosis.
The formula:
Normal vessel area - residual area of stenosis site / normal vessel area × 100 = percentage of stenosis.
The direct criteria of stenosis:
a.
Reduction in the diameter of the major light.
b.
Peak systolic velocity greater than 400 cm/s (at the site of stenosis).
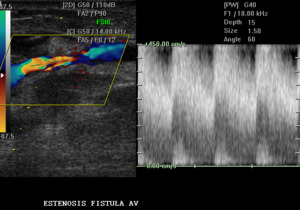
Fig. 18: Arteriovenous fistula is observed with increased velocities. SPV: 450 cm / s, compatible with AVF stenosis.
The indirect criteria are:
a.
Morphology of the high-resistance spectral wave before stenosis.
b.
Reduction in the volume of access flow.
c.
Aliasing artifact at the site of stenosis.
- Thrombosis
Thrombosis is the most common cause of vascular access failure; they're acute complications in the creation of the fistulas due to inadequate flow due to access or due to lack of adequate dilatation; thrombosis is rare in mature fistulas.
Doppler is the non-invasive method of choice for diagnosis,
we can observe the intraluminal thrombus of different echogenicities,
depending on its evolution,
not being able to compress the vein,
there're indirect methods for the suspicion of thrombosis as they are a pattern of high previous resistance to the site of thrombosis and decrease in systolic peak velocity posterior to the thrombosis site.
- Arterial steal
Arterial thefts in AVF are relatively frequent.
They're clinically characterized by pain at rest,
pain during hemodialysis sessions,
pallor of the extremities.
The diagnosis is easy to demonstrate by Doppler,
it consists of evaluating the nutritional artery in its segments proximal and distal to the anastomosis,
evidencing a change in the direction of flow in the color Doppler in the distal segments.
- Other complications
Another possible complication is the formation of pseudoaneurysms,
which develop mainly at the site of anastomosis or at the repetitive puncture sites,
are clearly identified by color Doppler ultrasound as saccular dilatations with the sign "yin-yang" and bidirectional flow.
The measurement of the neck,
the size of the pseudoaneurysm and whether there is associated thrombosis or peripheral hematoma should be evaluated.
Fig. 19: Pseudoaneurysm: a pulsatile collection is seen, located laterally to the fistula, with the sign of yin yang in Color Doppler, and the flow that enters and leaves through a union zone called neck of the sac.
Fig. 20: Schematic representation of a pseudoaneurysm formation, with bidirectional flow of in and out, observed in color scale with Doppler ultrasound. It is filled in systole and emptied in diastole.

Fig. 21: Hypoechoic image is observed with content inside adjacent to AVF, compatible with collection.
The adequate knowledge for the correct evaluation of arteriovenous fistulas,
by means of Doppler Color ultrasound,
from its planning,
pre and post-surgical follow-up,
monitoring,
follow-up and its complications,
allow the decision making in the creation of a vascular access and its success,
the role played by the radiologist is fundamental,
the pillar being therapy for the treatment of patients with renal replacement.
We show several cases with patients of our institution with arteriovenous fistulas and their evaluation with color Doppler ultrasound.
We identify mature and functioning AV fistulas,
as well as those at risk of failure,
poor prognosis and with multiple early complications.


. The humeral artery is observed with a spectrum of low resistance and high velocities. VPS: 100 cm/s")











