Spinal dysraphism includes wide range of pathologies occurring due to aberrations in development of spinal cord.
Spinal cord development includes three phases namely gastrulation,
primary neurulation and secondary neurulation.
Gastrulation involves conversion of the bilaminar embryonic disk to a trilaminar disk composed of ectoderm,
mesoderm,
and endoderm.
Another critical event occurring along with gastrulation is the formation of notochord,
cylindrical structure of mesodermal origin.
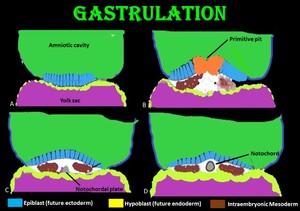
Fig. 2: Gastrulation and Development of notochord: (A) Coronal view through the bilaminar disc (B) Epiblast cells invaginate at the primitive pit creating the cells of the definitive endoderm as well as the mesoderm (C)Formation of definitive intra-embryonic mesoderm and notochordal plate (D) Notochordal plate then detaches from the endoderm, and forms a tube referred to as the definitive notochord.
Primary neurulation involves closure of neural plates to form neural tube.
Notochord invites the ectodermal cells to differentiate into neural precursor cells,
forming the neural plate.
Closure of neural tube begins at the medial hinge point in the ventral midline.
Fusion proceeds in both rostral and caudal directions.
During closure unfused rostral and caudal regions are referred as neuropores.
Neural crest cells at the lateral border of neural plates,
separates from the neural tube during closure and forms a mass dorsal to neural tube.
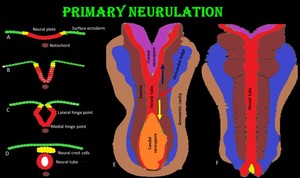
Fig. 3: Primary neurulation: The neural tube (red) and neural crest cells (yellow) are derived from surface ectoderm which forms neural plate induced by notochord (brown). (A)Future neural crest cells reside lateral to future neural tube. (B) Beginning of neural plate folding and internalization of neural plate cells. (C) Medial and lateral hinge plate facilitating folding of neural plate. (D) Separation of neural crest cells to form a mass dorsal to neural tube. (E) and (F) Dorsal view showing the closure of neural tube which begins in the center and progress in both cranial (blue arrow)and caudal (yellow arrow)direction.
Secondary neurulation involves the formation of conus medullaris and filum terminale.
The neuroepithelial cells of closed neural tube forms primitive nerve cells called neuroblast.
Neuroblasts forms the mantle layers and axons proceeding in and out of the mantle layers forms the marginal layer which becomes grey and white matter respectively.
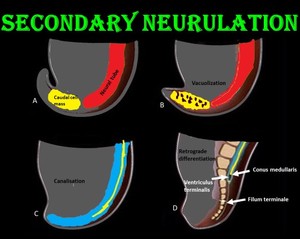
Fig. 4: Secondary neurulation: (A & B) Formation and vacuolization of caudal cell mass from the caudal end of neural tube distal to caudal neuropore. (C) Coalition of vacuoles and connection to the central canal by canalization. (D) In retrograde differentiation, cells of caudal cell mass undergo apoptosis to form conus medullaris, filum terminale and ventriculus terminalis.
Vertebral column is formed from the intraembryonic mesoderm as described below.
Remnants of notochord make up nucleus pulposus at the center of the intervertebral disc.
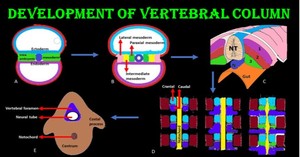
Fig. 5: Vertebral column development: (A) Intraembryonic mesoderm is located between the ectoderm and endoderm except where the notochord is found. (B) Intraembryonic mesoderm differentiates into paraxial , intermediate and lateral mesoderm. (C) Paraxial mesoderm divides into segments called somites, which divides into 3 parts dermatome [1], myotome [2] and sclerotome [3]. Vertebral column develops from sclerotome. (D & E) Each sclerotome divides into cranial and distal part. Caudal part will fuse with the cranial part from next sclerotome and grow ventrally under the notochord and fuse to form centrum & grow dorsally around the neural tube to form the arches.
Spinal dysraphism can be classified based on embryological events as shown below.
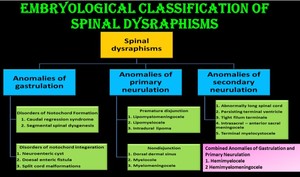
Fig. 6: Embryological classification of Spinal Dysraphisms
Evaluation of patient with spinal dysraphism begins with clinical assessment.
The child’s back should be evaluated to look for presence/absence of skin covering,
back mass and cutaneous stigmata of dysraphism.
Patients with hypertrichosis,
atypical dimples,
true tails,
lipomas,
hemangiomas,
aplasia cutis or scar,
dermoid cyst or sinus have high index of suspicion for spinal dysraphism.
Patients suffer from difficulty with locomotion,
exhibit bladder dysfunction,
sensory disturbances,
orthopedic deformities of the lower extremities,
and back pain.
