For neonatal patients with heart disease,
cardiac X-ray computed tomography (CT) examinations are generally performed as the first choice of radiological examinations. Currently,
cardiac CT examinations are applied in many hospitals because it is possible to perform the procedure in a relatively short time when compared to magnetic resonance imaging examination and nuclear medicine examination. As shown in Fig.
1,
the cardiac CT examination can be performed by rapidly injection of a contrast agent with the adequate imaging timing based on heart rate information from an electrocardiogram [1]. Based on basic protocol,
various protocols to obtain good imaging quality has been proposed,
therefore management of X-ray exposure dose has become complex; unfortunately,
exposure doses during cardiac CT are known to be high [2].
In addition,
neonates are known to be more sensitive to radiation than adults,
many studies point out that the dose exposure to neonates is increasing due to the high frequency of the neonatal cardiac CT examination [3,4].
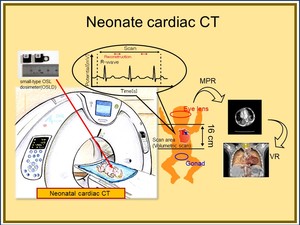
Fig. 1: Schematic drawing of the cardiac CT for neonate. The cardiac CT is useful to obtain clinical information, and we plan to measure the exposure dose during actual examinations.
For cardiac CT,
some imaging techniques have been proposed.
It is well-known that the helical scan mode is traditionally applied [5],
and recently volumetric scan mode can be used when a CT has wider area detector [6]. A 320-rowdetector CT is commercially available by Canon Medical Systems Corporation.
Figure 2 shows a comparison of scan modes between helical and volumetric scans. The volumetric scan can obtain the cardiac image using only one rotation of X-ray tubes; this means the image can be obtained without movement of the scanning bed.
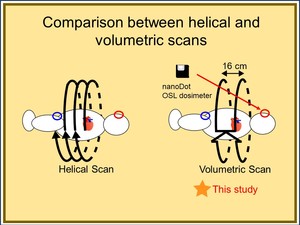
Fig. 2: Comparison between helical and volumetric scans. Small-type OSL dosimeter named nanoDot is suitable to measure actual dose. In this study, we focused our attention on the volumetric scan mode.
In order to reduce exposure dose during cardiac CT examination,
a system called “Automatic Exposure Control” (AEC) has been adopted for CT examination [7],
and suitable medical images can be obtained without information concerning the physical constitution of each patients. However,
from the viewpoint of radiation dosimetry,
it is difficult to manage exposure doses because of the intensity of exposing X-rays are varied based on the physical constitution of each patient. Therefore,
in order to solve such problems,
we considered that the exposure dose should be managed by actual dose measurement method.
As shown in Fig.
3,
the radiation doses inside the irradiation field are evaluated using the CT Dose Index (CTDI) [8].
On the other hand,
it is difficult to evaluate the exposure dose of the organs positioned outside the irradiation field such as the gonads and the eye lens. In this study,
we focused our attention on exposure dose measurements of sensitive organs outside the irradiation area. We performed actual dose measurement using a small-type optically stimulated luminescence dosimeter (OSLD) called nanoDot [9-11]. The nanoDot OSL dosimeter has the following favorable characteristics shown in Fig.
4; first,
the dosimeter is very small,
second,
it is not expensive,
third,
it is easy to wear,
and fourth,
the dosimeter has low detection efficiency and dosimetry on the order of 1 mGy is also possible; the last feature is most important when using the OSLD during actual clinical examinations,
because the dosimeter has a low detection efficiency,
it does not interfere with medical images. As discussed above,
the nanoDot OSL dosimeter is considered to be suitable for use during CT scanning.
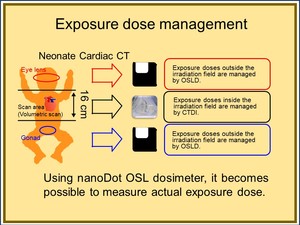
Fig. 3: Current exposure dose management during cardiac CT of a neonate. Exposure doses of organs outside the scan area are generally not evaluated. Therefore, we evaluated those areas using a small-type OSL dosimeter.
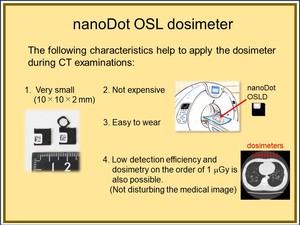
Fig. 4: Characteristics of the nanoDot OSL dosimeter. We think the OSL dosimeter is suitable forclinical examination application.
A procedure for deriving entrance surface dose (ESD) from response of OSL is presented in Fig.
5. Using a reading device for the dosimeter called microStar,
the intensity of the luminescence which is proportional to the exposure dose can be acquired and measured as “counts”.
Counts should be corrected by e,
which is the detection efficiency.
This value is provided by the manufacturer. The value of counts/e is converted to ESD using a dose calibration curve which was proposed by Takegami et al.
[10].
A calibration curve is shown in the lower part in Fig.
5. From this calibration curve,
the ESD can be obtained with an accuracy of 15% taking into consideration various factors such as angle dependence,
energy dependence,
and difference of detection efficiency; namely,
when applying the 15% uncertainty,
in diagnostic X-ray,
we should not consider the response of dosimeter concerning these factors. In this study,
we measured scattered X-rays during CT examination.
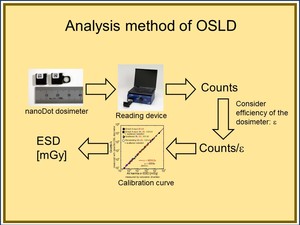
Fig. 5: A procedure for deriving ESD using the nanoDot OSL dosimeter. A reading device can obtain “counts” which are proportional to the amount of optically stimulated luminescence, therefore the counts can be converted to entrance surface dose (ESD) using a calibration curve.
The purpose of this study is to clarify exposure dose outside the irradiation area during neonatal cardiac CT examination.
Figure 6 shows an outline of this research toward clinical application. We performed a phantom study because we wanted to analyze the contribution of exposure doses and based on these data we want to fabricate novel X-ray shielding items for dose reduction to sensitive organs. At present,
there are few protective products for eye lenses and gonads during neonatal cardiac CT examination,
and it is necessary to develop appropriate shields for these organs [12,13].
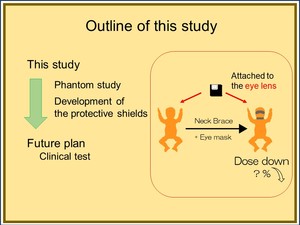
Fig. 6: Outline of this study. In this study, we performed a phantom study, our goal was to measure exposure doses and additionally we want to develop protective shields.






 using a calibration curve.")
