ECR 2019 / C-1885
Porta hepatis: Pandora’s Box, what the radiologist needs to know.
Congress:
ECR 2019
Poster Number:
C-1885
Type:
Educational Exhibit
Keywords:
Education and training, Education, Diagnostic procedure, Ultrasound, MR, CT, Abdomen
Authors:
M. AbouRayan1, M. T. El-Diasty2, F. Serag El-Din1; 1Alexandria/EG, 2Jeddah/SA
DOI:
10.26044/ecr2019/C-1885
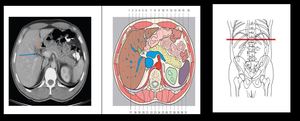
, CHA (blue arrow) & PV (black arrow) References: Moeller TB, Reif E. Pocket Atlas of Sectional Anatomy. 3rd ed. Thieme; 2007.")
Fig. 1:
Axial CT image and corresponding colored illustration at the level of porta...

Fig. 2:
Porta Hepatis; sagittal cross section diagram and corresponding MRI.