ECR 2019 / C-1893
Applying CT/MRI LI-RADS v2018 imaging features in interpreting liver MRI of patients at risk of HCC: a simplified approach for the juniors
Congress:
ECR 2019
Poster Number:
C-1893
Type:
Educational Exhibit
Keywords:
Multidisciplinary cancer care, Education and training, Education, Diagnostic procedure, MR, Liver, Abdomen
Authors:
M. T. El-Diasty1, M. Wazzan1, H. Sadec2, M. AbouRayan3, M. M. A. Rezk4, A. Abduljabbar1; 1Jeddah/SA, 2Alexandria /EG, 3Alexandria/EG, 4Cairo/EG
DOI:
10.26044/ecr2019/C-1893

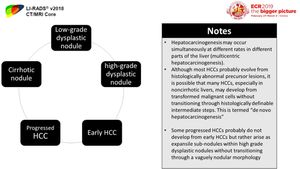
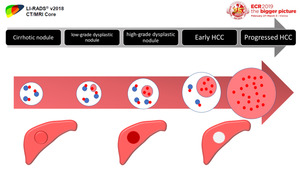
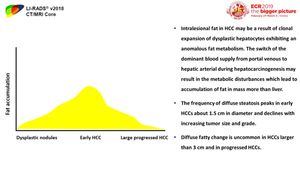
Fig. 2:
Different pathological stages of hepatocarcinogenesis
 arteries and decrease of the portal flow with the development of arterial phase hyperenhancement.")
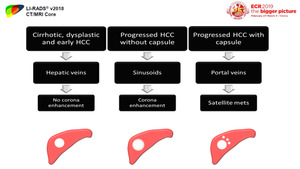
Fig. 3:
Diagram shows the progressive increase of unpaired (nontriadal) arteries and...
, progressed HCCs without fibrous capsules and progressed HCCs with fibrous capsules.")
Fig. 4:
Diagram shows the difference in venous drainage between cirrhotic (nodules,...

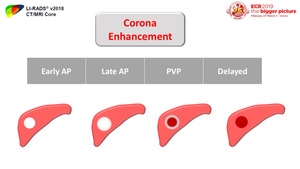
Fig. 5:
"Corona enhancement" is the peritumoral parenchymal enhancement that begins a...

Fig. 6:
Diagram and axial post contrast axial T1 image in PV phase show the capsule...

Fig. 7:
The frequency of diffuse intranodular steatosis increases from low-grade...

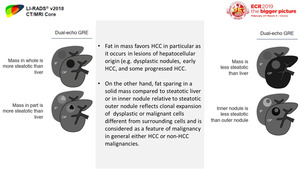
Fig. 8:
Difference of fat deposition in a mass more than the surrounding liver and fat...

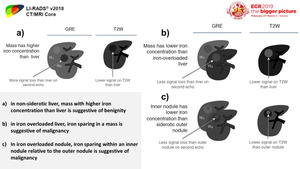
Fig. 9:
Iron resistance is observed also in dysplastic foci, dysplastic nodules, and...

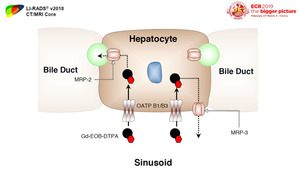
Fig. 10:
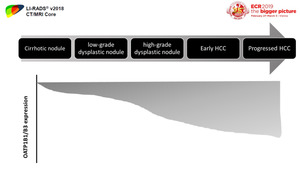
OATP1B1/B3 is one of these transporters that is suggested to be responsible for...

Fig. 11:
Diagram shows reduction in OATP expression during hepatocarcinogenesis

Fig. 12:
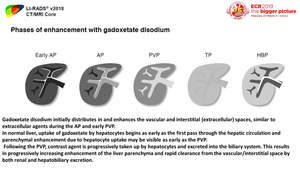
The degree of gadoxetate uptake by a lesion depends on the expression and...