ECR 2019 / C-1993

Functional Outcome of Temporal Lobe Epilepsy Surgery based on Memory Functional MRI
Congress:
ECR 2019
Poster Number:
C-1993
Type:
Scientific Exhibit
Keywords:
Neuroradiology brain, MR-Functional imaging, Diagnostic procedure, Seizure disorders
Authors:
V. Sawlani, K. Kawsar, D. McCorry, A. Hawkins, J. Herbert, R. Chelvarajah; Birmingham/UK
DOI:
10.26044/ecr2019/C-1993

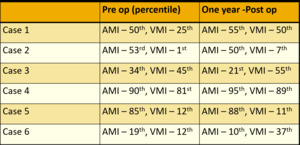
Fig. 4:
Pre and post operative Auditory and Visual Memory Index

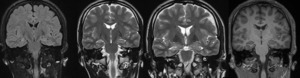
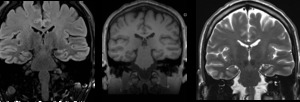
Fig. 5:
Case 1. Coronal FLAIR, T2W and T1W MRI shows unequivocal appearances of right...

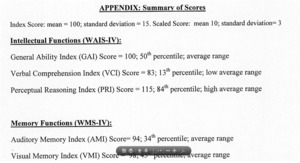
Fig. 6:
Case 1. Pre-operative neuropsychological assessment showed average intellectual...
, (left > right), activation of secondary visual cortex, parietal cortex, dorsolateral prefrontal cortex and anterior language areas.")
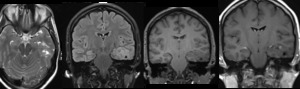
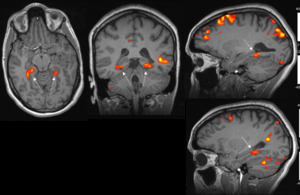
Fig. 7:
Case 1. Memory fMRI – Imaginary Walk Paradigm Day 1 shows Bilateral...
.")
Fig. 8:
Case 2. Low grade glioma in the left medial temporal lobe involving the...
.")
Fig. 9:
Case 2. Memory fMRI – Imaginary Walk Paradigm shows almost symmetrical...
- Lesionectomy and radical Hippocampectomy performed.")
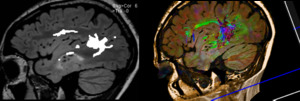
Fig. 10:
Case 2. ECOG guided surgery with DTI (Arcuate fasciculus)- Lesionectomy and...

Fig. 11:
Case 3. MRI shows left-sided hippocampal sclerosis.
.")
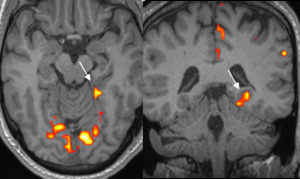
Fig. 12:
Case 3. Day 1 imaginary Walk Paradigm shows activation only in left...
, anterior language areas, dorsolateral prefrontal cortex, and secondary visual cortex.")
Fig. 13:
Case 3. Day 2 fMRI examination shows similar activation in left...