MVT is an uncommon disease,
it represents between 5% and 20% of episodes of mesenteric ischemia,
depending on the literature consulted.
It's potentially lethal,
between 12.5-50% of complicated cases with intestinal infarction die.
MVT presents with nonspecific symptoms and the diagnostic delay worsens the prognosis.
CT is a sensitive,
specific,
rapid,
non-invasive and available imaging technique.
Classification of MVT according to the cause:
- Primary: idiopathic,
without risk factors.
- Secondary (most frequent) to:
Intra-abdominal pathology:
- Abdominal surgery,
closed abdominal trauma.
- Inflammatory/infectious diseases: pancreatitis,
inflammatory bowel disease,
diverticulitis,
appendicitis,
intra-abdominal sepsis.
- Intestinal obstruction: volvulus, intestinal intussusception.
- Portal hypertension: cirrhosis,
splenectomy,
splenomegaly,
endoscopic sclerotherapy of varicose veins.
Hypercoagulability states:
- Peripheral deep venous thrombosis,
pregnancy,
oral contraceptives,
neoplasms,
myeloproliferative syndromes,
sickle cell disease,
polycythemia vera,
anticardiolipin antibodies,
lupus anticoagulant, factor V Leiden,
hyperfibrinogenemia,
C and S protein deficiency,
antithrombin III deficiency,
resistance to tissue plasminogen activator.
Intestinal venous drainage:
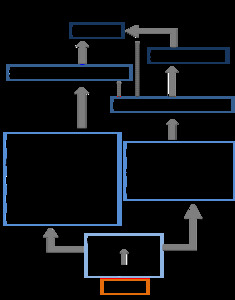
Fig. 1: Intestinal venous drainage scheme.
Fig. 2: Main veins of mesenteric venous drainage.
The location of the thrombus in the mesenteric venous system usually depends on the etiology of the process:
- Intra-abdominal cause of MVT: the tendency of the thrombus is to locate proximally (portomesenteric confluence) and to progress distally.
- Hematologic cause: predilection of the thrombus to be located in distal venous branches and progressing proximally.
Diagnosis of MVT:
The clinical presentation is nonspecific and depends on the evolution of MVT:
- Acute MVT: less than 1 month of evolution (most common 48h).
- Diffuse and nonspecific abdominal pain.
- Nausea,
vomiting.
- Diarrhea/constipation.
- Digestive hemorrhage.
- Abdominal distention (may indicate acute mesenteric ischemia)
Clinical suspicion of acute MVT is fundamental and is based on a disproportionate abdominal pain to the physical examination with or without risk factors.
- Chronic MVT: more than 1 month of evolution.
- Asymptomatic (incidental)
- Debut: Complications of portal hypertension (bleeding of varicose veins).
- Weight loss/appetite.
- Postprandial pain.
Complementary tests:
- Analytical: nonspecific,
leukocytosis,
metabolic acidosis if intestinal necrosis.
- SimpleX-ray: nonspecific.
- Ultrasound: explorer-dependent, technical difficulties (gas interposition, low acoustic window).
- MR: low availability in urgency.
- Contrast-enhanced CT: is the imaging technique of choice for the diagnosis of MVT (non-invasive,
high sensitivity,
specificity,
speed and availability).
- Venous repletion defect (central hypodensity).
- Parietal enhancement of the affected venous segment.
- Increased venous caliber at the thrombus level (acute MVT).
- Congestion of mesenteric veins.
- Mesenteric edema (striation of mesenteric fat and free fluid) secondary to transudation due to venous obstruction.
- Collateral venous circulation (chronic MVT).
- CT findings of intestinal involvement associated with MVT:
- Regular and circumferential wall thickening (most frequent): edematous and/or intramural hemorrhage.
- Submucosal hyperdense on CT without and with contrast: intramural hemorrhage.
- Target sign: mucosa and muscle enhancement due to hyperemia and hypodense submucosa due to edema.
- Mural enhancement due to venous congestion of the intestinal wall.
- Absence of mural enhancement with intravenous contrast.
- Bowel distension (aperistaltic loops).
- Pneumatosis intestinalis.
- Portal / mesenteric venous gas.
- Pneumoperitoneum: perforation of infarcted loops.
- Angiography: it's diagnostic and therapeutic,
but invasive technique,
so it's used in selected cases (non-diagnostic CT in cases of high clinical suspicion of MVT).
Complications of MVT:
- The greatest severity lies in the complication of MVT with intestinal ischemia,
which occurs more frequently in acute processes,
when the thrombus is located distally and when there is a greater extent of thrombosis.
- The development of collateral venous circulation translates complication with portal hypertension and hemorrhagic varices,
which occurs more frequently when the process is chronic,
the location of the thrombus is proximal and the extent of the thrombus is smaller.
Pathogeny of the complications of MVT:
- Acute MVT→ Venous congestion of the intestinal wall and conserved arterial flow → Increase in capillary hydrostatic pressure (intestinal wall edema) → Decrease in arterial supply → Ischemia and intestinal infarction
- Chronic TVM → Decreased portal flow → Compensating hepatic arterial vasodilation and collateral venous circulation → Cavernous transformation of the portal vein → Portal hypertension → Hemorrhagic varices,
portal cholangiopathy
Treatment:
- Anticoagulation (treatment of choice): immediate,
for 6-12 months,
decreases recurrence and mortality.
- Surgery (intestinal resection limited to the necrotic segment) with anticoagulation: indicated when we observed a central venous hypodensity with intestinal parietal thickening and free peritoneal fluid,
signs of peritonitis and / or signs of intestinal ischemia.
- Surgical thrombectomy when the acute thrombus is located proximally in the superior mesenteric vein.
- Thrombolysis with urokinase,
streptokinase,
t-PA: systemic,
percutaneous transjugular or transhepatic,
transarterial.
- Indefinite anticoagulation when there are hypercoagulable states.
- Do not treat asymptomatic chronic VMT.


